

Nerve root compression due to lumbar spinal canal tophi: A case report and review of the literature
- PMID: 36397389
- PMCID: PMC9666167
- DOI: 10.1097/MD.0000000000031562
Nerve root compression due to lumbar spinal canal tophi: A case report and review of the literature
Abstract
Rationale: Gout in the spine and adnexa is rare in clinical practice and can also be easily misdiagnosed, we reported a patient with nerve root compression due to lumbar gout stones in the lumbar spinal canal.
Patient concerns: A 51-year-old male was admitted to the hospital with lumbar pain with numbness in the left lower limb for more than 6 months. The physical examination showed that tenderness and percussion pain were present at L4-S1 spinous process. Straight leg raise test: 50° on the left side were positive. Laboratory tests showed that the sUA was 669 μmol/L, MRI of the lumbar spine showed that cystic T1WI low signal and T2WI mixed high signal shadows were seen in the spinal canal at the level of L4-L5.
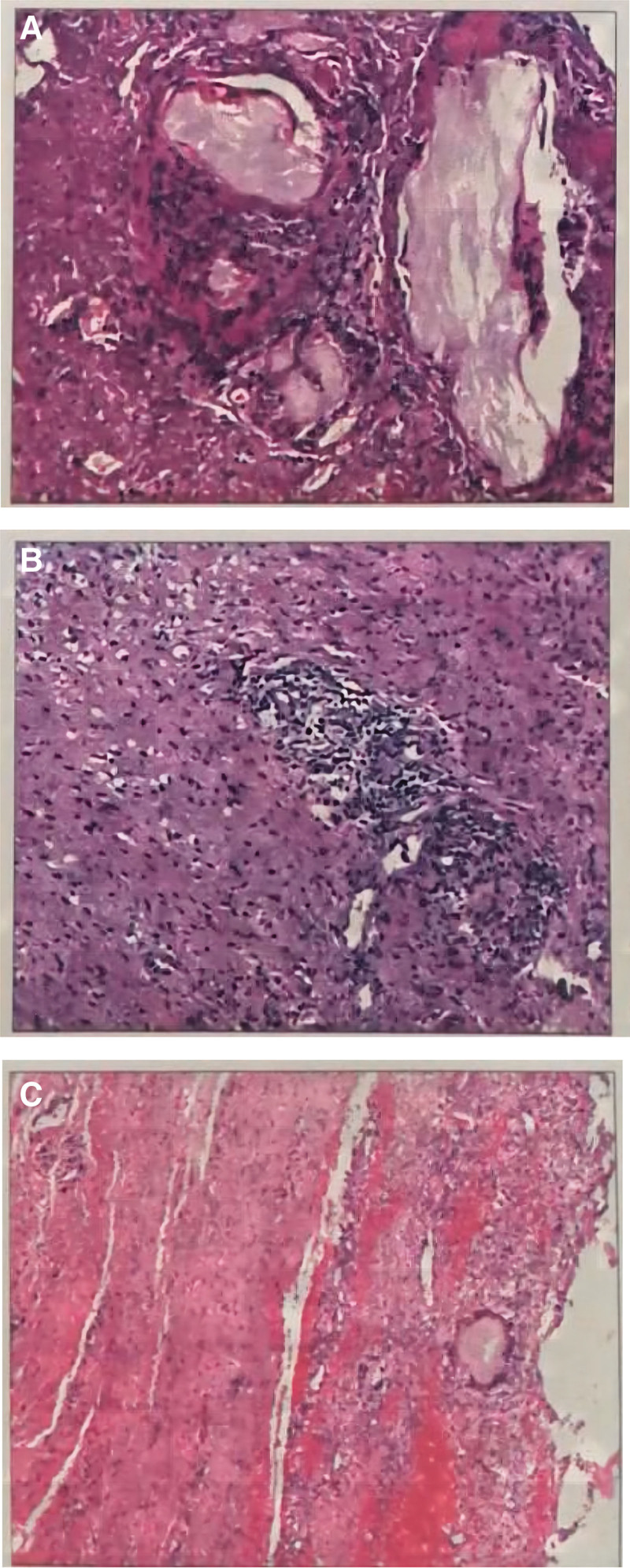
Diagnoses: Combining with lab examinations, imaging examinations, and histopathological results, the patient was diagnosed with lumbar spinal canal tophi.
Interventions: After active improvement of all examinations, the patient underwent surgical treatment with decompression and internal fixation of the L4-L5 segment.
Outcomes: After surgery, the patient's symptoms improved and muscle strength returned to normal. Among the 95 previously reported patients with lumbar gout, the ratio of men to women was 2.96:1, and the peak age group of incidence was 56 to 65 years. The onset of the disease was mainly in a single segment of the lumbar spine, with 34.41% of all cases occurring at the L4-L5 level. 61.05% of the patients had a history of gout attacks or hyperuricemia, and the most frequently involved site was the foot and ankle, followed by the wrist. Sixty-seven patients underwent surgical treatment, and 22 chose conservative treatment, with overall satisfactory results.
Lessons subsections: The incidence of lumbar gout is low and relatively rare in the clinic and pathological biopsy is still the gold standard. Vertebral plate incision and decompression are often selected for surgical treatment, and whether to perform fusion should be comprehensively considered for the destruction of vertebral bone by gout and the reasonable selection of the extent of surgical resection. Whether choosing surgical treatment or conservative therapy, the control of uric acid levels should be emphasized.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures










References
-
- Luo H, Fang W, Zuo X, et al. Analysis of clinical characteristics, diagnosis and treatment of gout patients in China. Chin J Intern Med. 2018;57:27–31. - PubMed
-
- Hou LC, Hsu AR, Veeravagu A, et al. Spinal gout in a renal transplant patient: a case report and literature review. Surg Neurol. 2007;67:65–73; discussion 73. - PubMed
-
- Qin DA, Song JF, Li X-F, et al. Tophaceous gout of lumbar spine with fever mimicking infection. Am J Med. 2018;131:e353–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
