

Combination conventional endoscopy and endoscopic ultrasound can differentiate between esophageal granular cell tumors and leiomyomas
- PMID: 36397402
- PMCID: PMC9666135
- DOI: 10.1097/MD.0000000000031435
Combination conventional endoscopy and endoscopic ultrasound can differentiate between esophageal granular cell tumors and leiomyomas
Abstract
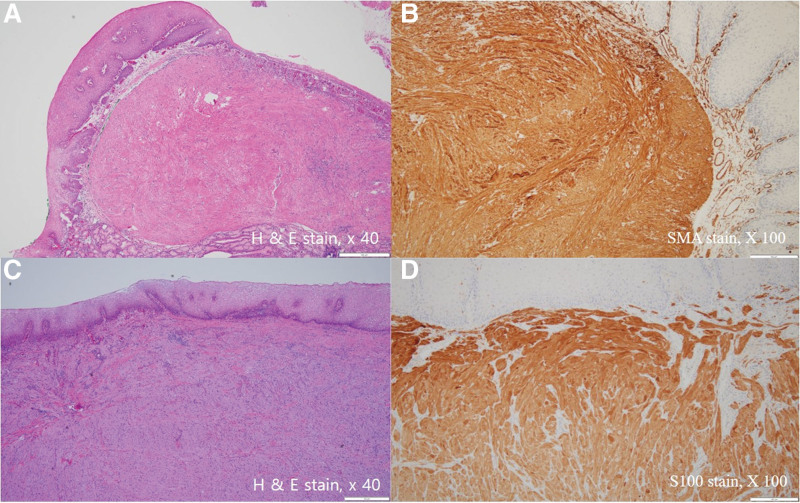
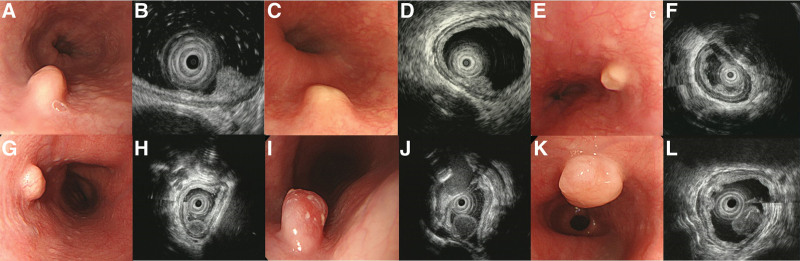
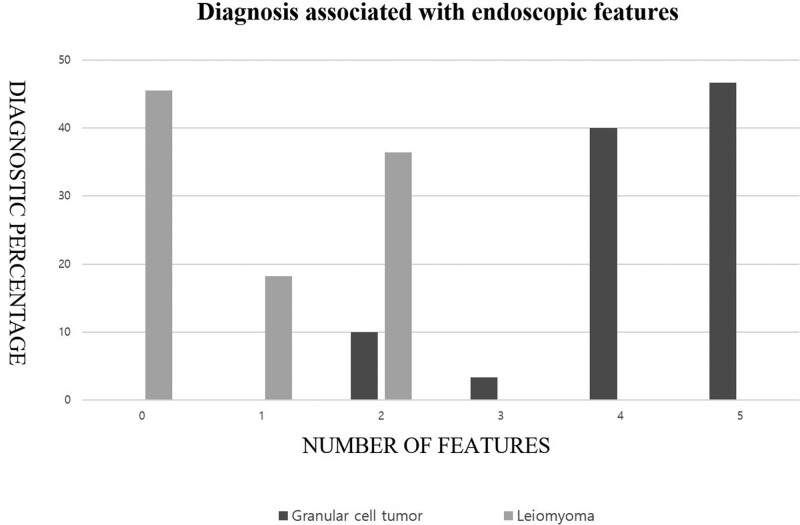
Esophageal leiomyomas and granular cell tumors (GCTs) are the 2 most common subepithelial tumors found in the esophagus. We attempted to differentiate the 2 tumors using endoscopic findings and endoscopic ultrasound (EUS) features. Between December 2008 and June 2021, a total of 38 esophageal GCTs and 11 esophageal leiomyomas originating from the muscularis mucosa were selected. Clinical characteristics and endoscopic features were retrospectively reviewed. Although esophageal GCTs are mainly located in the lower third of the esophagus (81.6%), esophageal leiomyomas are mainly located in the upper third of the esophagus (45.5%). Broad-based (84.2%, P = .002) and whitish-to-yellowish color changes (97.4%, P < .001) are significant endoscopic features of esophageal GCTs. The echogenicity of esophageal leiomyoma was similar to that of proper muscle echogenicity. However, the echogenicity of esophageal GCTs was hyperechoic compared to that of the proper muscle layer (90.0% vs 9.1%, respectively, P < .001). EUS revealed a clearer hyperechoic epithelial lining in the esophageal leiomyoma than in esophageal GCTs (100% vs 26.7%, respectively, P < .001). The 5 endoscopic factors (location of the lower third, broad base, whitish-to-yellowish color, hyper-echogenic, and unclear demarcated hyperechoic epithelial line) were counted to differentiate esophageal GCTs from esophageal leiomyomas. Tumors with 3 or more endoscopic factors were all esophageal GCTs. The characteristic endoscopic and EUS features of esophageal GCTs were broad-based, whitish-to-yellowish colored subepithelial tumors located in the lower third of the esophagus and hyperechoic tumor with an unclear demarcated hyperechoic epithelial line. A combination of these features can predict esophageal GCTs before endoscopic resection.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
The diagnostic value of endoscopic ultrasound for esophageal subepithelial lesions: A review.Medicine (Baltimore). 2024 Nov 15;103(46):e40419. doi: 10.1097/MD.0000000000040419. Medicine (Baltimore). 2024. PMID: 39560558 Free PMC article. Review.
-
Endosonographic features of esophageal granular cell tumors using a high-frequency catheter probe.Scand J Gastroenterol. 2011 Feb;46(2):142-7. doi: 10.3109/00365521.2010.525661. Epub 2010 Oct 18. Scand J Gastroenterol. 2011. PMID: 20950209
-
Esophageal Granular Cell Tumors Can Be Differentiated from Leiomyomas Using Endoscopic Ultrasonography.Intern Med. 2018 Jun 1;57(11):1509-1515. doi: 10.2169/internalmedicine.9816-17. Epub 2018 Jan 11. Intern Med. 2018. PMID: 29321437 Free PMC article.
-
Clinical outcomes of esophageal granular cell tumors with different endoscopic resection methods.Sci Rep. 2023 Jul 3;13(1):10738. doi: 10.1038/s41598-023-37998-x. Sci Rep. 2023. PMID: 37400629 Free PMC article.
-
Esophageal granular cell tumors: report of 9 cases and a literature review.World J Gastroenterol. 2012 Dec 21;18(47):7118-21. doi: 10.3748/wjg.v18.i47.7118. World J Gastroenterol. 2012. PMID: 23323018 Free PMC article. Review.
Cited by
-
The diagnostic value of endoscopic ultrasound for esophageal subepithelial lesions: A review.Medicine (Baltimore). 2024 Nov 15;103(46):e40419. doi: 10.1097/MD.0000000000040419. Medicine (Baltimore). 2024. PMID: 39560558 Free PMC article. Review.
-
Slicing Through the Options: A Systematic Review of Esophageal Leiomyoma Management.Cureus. 2025 Apr 2;17(4):e81614. doi: 10.7759/cureus.81614. eCollection 2025 Apr. Cureus. 2025. PMID: 40177232 Free PMC article. Review.
-
A Granular Cell Tumor Arising in a Patient with Long-segment Barrett's Esophagus.Intern Med. 2025 Feb 15;64(4):557-561. doi: 10.2169/internalmedicine.3933-24. Epub 2024 Jun 27. Intern Med. 2025. PMID: 38925966 Free PMC article.
References
-
- Rejas RA, Campos MS, Cortes AR, et al. . The neural histogenetic origin of the oral granular cell tumor: an immunohistochemical evidence. Med Oral Patol Oral Cir Bucal. 2011;16:e6–10. - PubMed
-
- Lee LS, Singhal S, Brinster CJ, et al. . Current management of esophageal leiomyoma. J Am Coll Surg. 2004;198:136–46. - PubMed
-
- Marolleau F, Baert F, Mertens V, et al. . Abrikossoff cell tumor of the oesophagus: a case report and review of the literature. Acta Clin Belg. 2008;63:273–6. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
