

Recurrence risk of venous thromboembolism associated with systemic lupus erythematosus: A retrospective cohort study
- PMID: 36397932
- PMCID: PMC9663318
- DOI: 10.1002/rth2.12839
Recurrence risk of venous thromboembolism associated with systemic lupus erythematosus: A retrospective cohort study
Abstract
Background: Recurrence risk of systemic lupus erythematosus (SLE)-associated venous thromboembolism (VTE) is unclear.
Aim: To determine the recurrence risk of SLE-associated VTE overall and by presence of provoking factors and SLE flares.
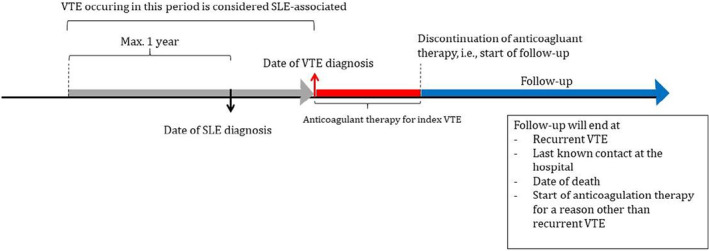
Methods: A multicenter, retrospective cohort study was conducted among patients with first SLE-associated VTE who discontinued anticoagulation. SLE flares were defined as Systemic Lupus Erythematosus Disease Activity Index 2000 greater than 4. The primary outcome was recurrent VTE. Incidence rates and cumulative incidences were calculated by presence of provoking factors and antiphospholipid syndrome (APS) at index VTE. The hazard ratio (HR) for recurrence after SLE flare-associated index VTE was estimated with Cox regression, adjusted for provoking factor presence and APS.
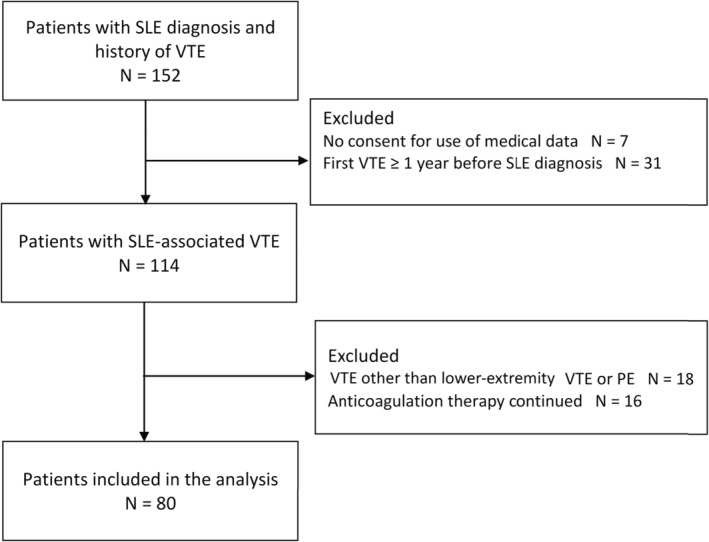
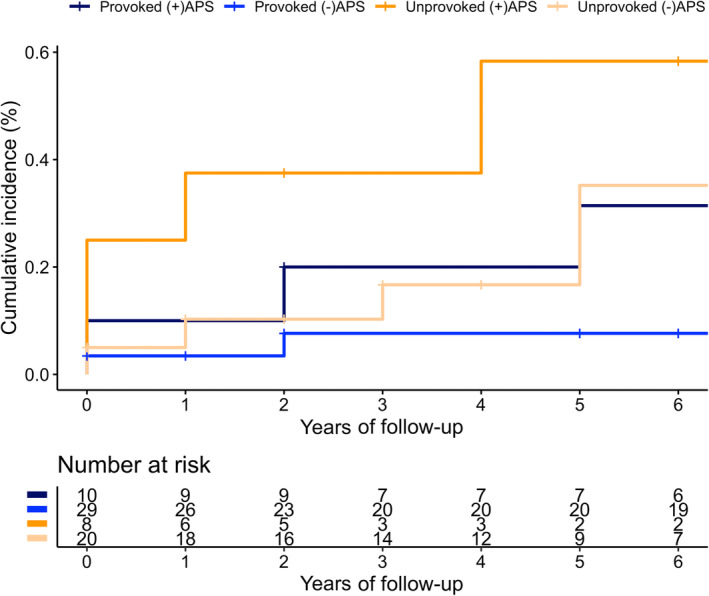
Results: Eighty patients were included with 21 recurrent VTEs in median 8 years. For provoked index VTE, the recurrence rate in patients without APS was 1.1 per 100 person-years (PY; 95% confidence interval [CI], 0.1-3.1) and in the presence of APS 3.5 per 100 PY (95% CI, 0.9-8.9), yielding cumulative incidences of 7.5% (95% CI, 1.2%-21.7%) and 31.4% (95% CI, 6.3%-61.6%) respectively. For unprovoked index VTE, these analogous rates were 3.8 per 100 PY (95% CI, 1.2-9.0) and 16.7 per 100 PY (95% CI, 4.5-42.7), with cumulative incidences of 33.7% (95% CI, 10.7%-58.9%) and 54.2% (95% CI, 10.7%-84.5%), respectively. Forty-six index VTEs were flare associated, and the adjusted HR for recurrence was 0.4 (95% CI, 0.1-1.8) compared to those without flares at their index VTE.
Conclusion: Antiphospholipid syndrome is the main determinant for recurrence risk of SLE-associated VTE irrespective of presence of a provoking factor. Future research should attempt to confirm that flare-associated VTE has a lower recurrence risk.
Keywords: antiphospholipid syndrome; inflammation; systemic lupus erythematosus; thrombosis; venous thromboembolism.
© 2022 The Authors. Research and Practice in Thrombosis and Haemostasis published by Wiley Periodicals LLC on behalf of International Society on Thrombosis and Haemostasis (ISTH).
Figures
References
-
- Baglin T, Bauer K, Douketis J, Buller H, Srivastava A, Johnson G. Duration of anticoagulant therapy after a first episode of an unprovoked pulmonary embolus or deep vein thrombosis: guidance from the SSC of the ISTH. J Thromb Haemost. 2012;10(4):698‐702. doi: 10.1111/j.1538-7836.2012.04662.x - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
