

Acalabrutinib Versus Investigator's Choice in Relapsed/Refractory Chronic Lymphocytic Leukemia: Final ASCEND Trial Results
- PMID: 36398134
- PMCID: PMC9666115
- DOI: 10.1097/HS9.0000000000000801
Acalabrutinib Versus Investigator's Choice in Relapsed/Refractory Chronic Lymphocytic Leukemia: Final ASCEND Trial Results
Abstract
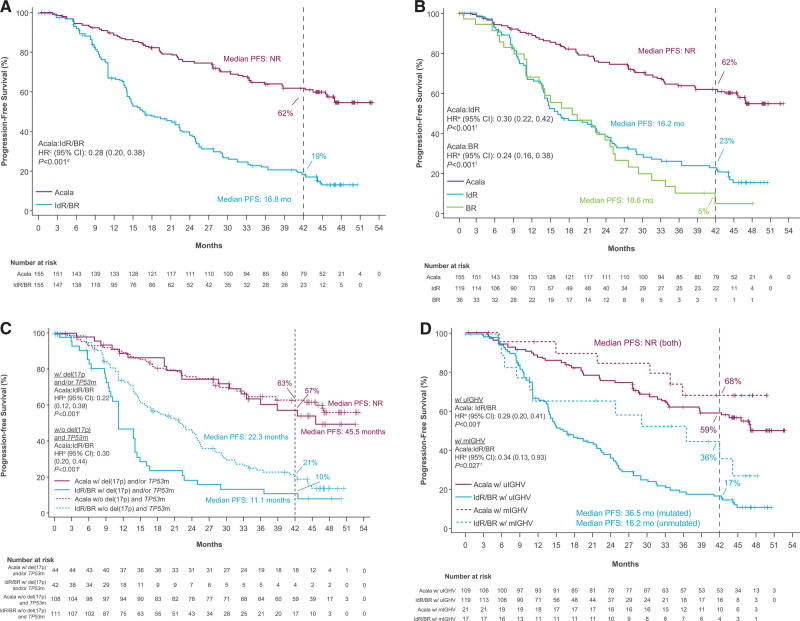
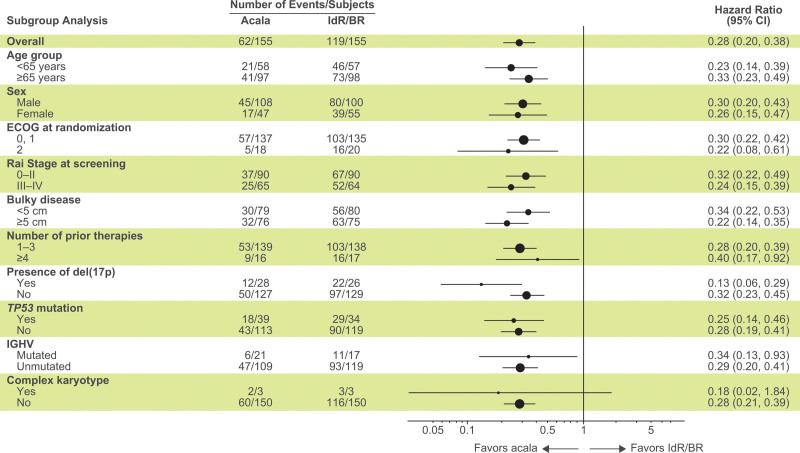
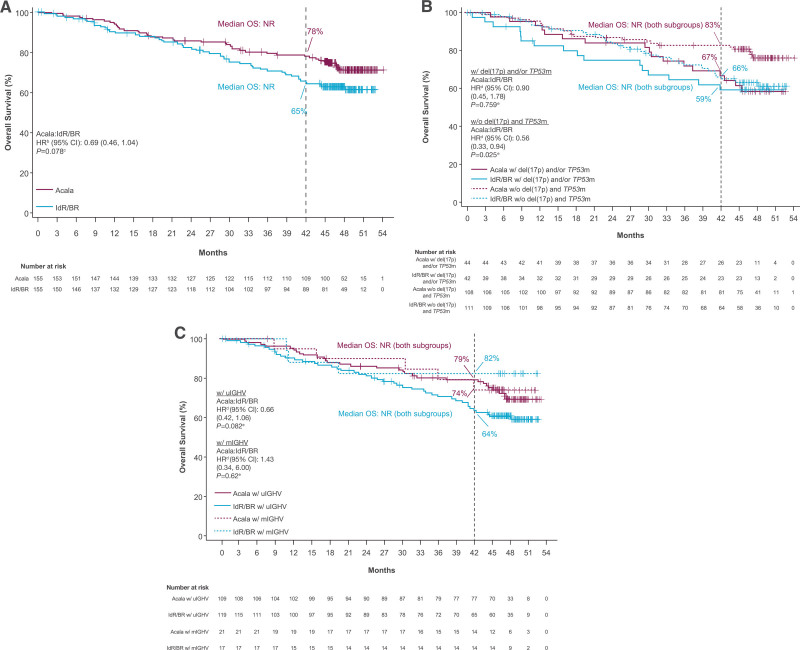
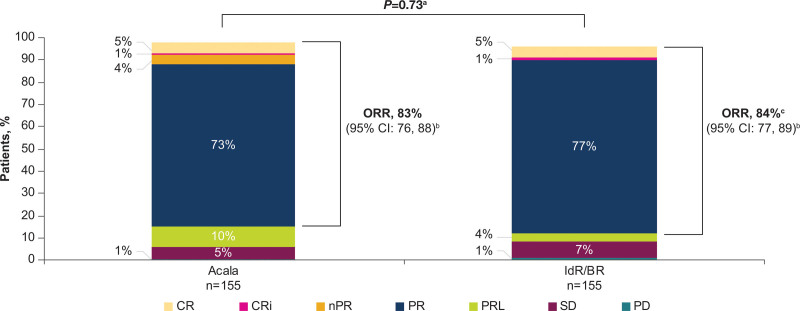
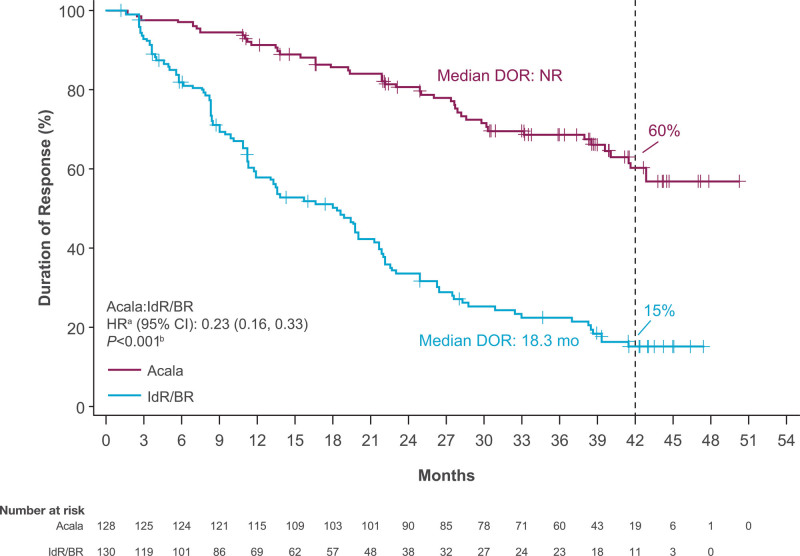
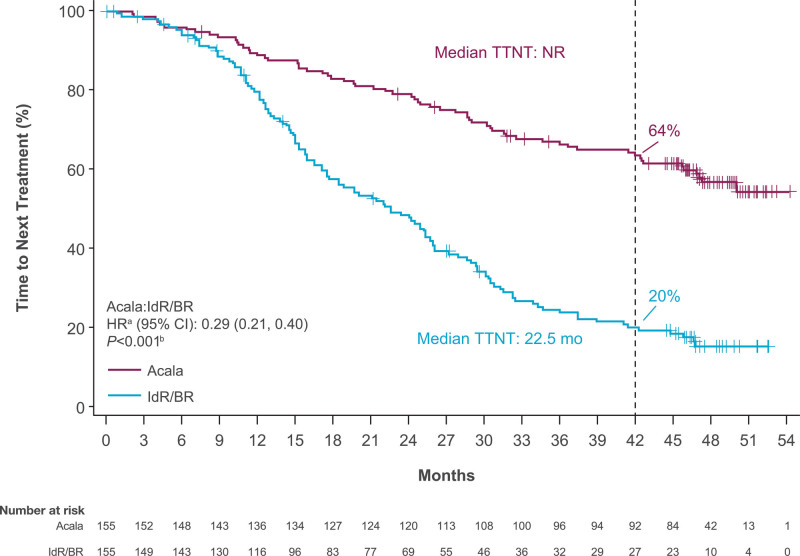
Acalabrutinib is a Bruton tyrosine kinase inhibitor approved for patients with chronic lymphocytic leukemia (CLL). ASCEND is the pivotal phase 3 study of acalabrutinib versus investigator's choice of idelalisib plus rituximab (IdR) or bendamustine plus rituximab (BR) in patients with relapsed/refractory (R/R) CLL. In the primary ASCEND analysis (median 16.1-month follow-up), acalabrutinib showed superior efficacy with an acceptable tolerability profile versus IdR/BR; here, we report final ~4 year follow-up results. Patients with R/R CLL received oral acalabrutinib 100 mg twice daily until progression or unacceptable toxicity, or investigator's choice of IdR or BR. A total of 310 patients (acalabrutinib, n = 155; IdR, n = 119; BR, n = 36) were enrolled. At median follow-up of 46.5 months (acalabrutinib) and 45.3 months (IdR/BR), acalabrutinib significantly prolonged investigator-assessed progression-free survival (PFS) versus IdR/BR (median, not reached [NR] vs 16.8 months; P < 0.001); 42-month PFS rates were 62% (acalabrutinib) versus 19% (IdR/BR). Median overall survival (OS) was NR (both arms); 42-month OS rates were 78% (acalabrutinib) versus 65% (IdR/BR). Adverse events led to drug discontinuation in 23%, 67%, and 17% of patients in the acalabrutinib, IdR, and BR arms, respectively. Events of clinical interest (acalabrutinib vs IdR/BR) included all-grade atrial fibrillation/flutter (8% vs 3%), all-grade hypertension (8% vs 5%), all-grade major hemorrhage (3% vs 3%), grade ≥3 infections (29% vs 29%), and second primary malignancies excluding nonmelanoma skin cancer (7% vs 2%). At ~4 years follow-up, acalabrutinib maintained favorable efficacy versus standard-of-care regimens and a consistent tolerability profile in patients with R/R CLL.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the European Hematology Association.
Figures
References
-
- Imbruvica [package insert]. Sunnyvale, CA, Horsham, PA: Pharmacyclics, Janssen Biotech, Inc.2022.
-
- Pellegrini L, Novak U, Andres M, et al. . Risk of bleeding complications and atrial fibrillation associated with ibrutinib treatment: a systematic review and meta-analysis. Crit Rev Oncol Hematol. 2021;159:103238. - PubMed
LinkOut - more resources
Full Text Sources