

Early vitrectomy for exogenous endophthalmitis following surgery
- PMID: 36398614
- PMCID: PMC9672977
- DOI: 10.1002/14651858.CD013760.pub2
Early vitrectomy for exogenous endophthalmitis following surgery
Abstract
Background: Endophthalmitis is a sight-threatening emergency that requires prompt diagnosis and treatment. The condition is characterised by purulent inflammation of the intraocular fluids caused by an infective agent. In exogenous endophthalmitis, the infective agent is foreign and typically introduced into the eye through intraocular surgery or open globe trauma.
Objectives: To assess the potential role of combined pars plana vitrectomy and intravitreal antibiotics in the acute management of exogenous endophthalmitis, versus the standard of care, defined as vitreous tap and intravitreal antibiotics.
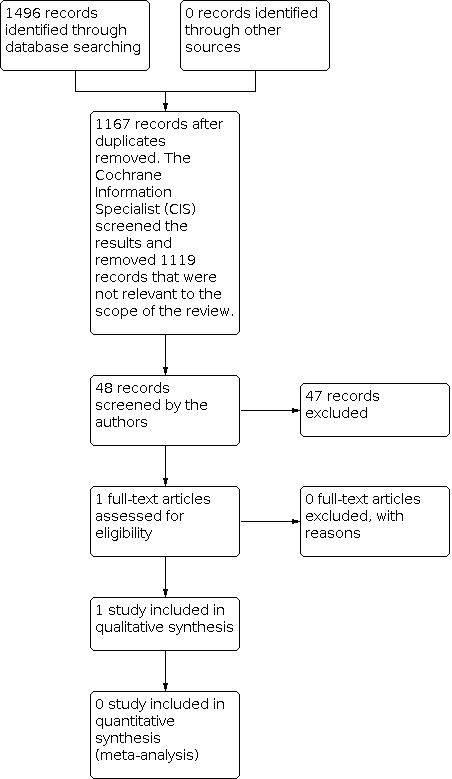
Search methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL; which contains the Cochrane Eyes and Vision Trials Register; 2022, Issue 5); Ovid MEDLINE; Ovid Embase; the International Standard Randomised Controlled Trial Number registry; ClinicalTrials.gov, and the World Health Organization International Clinical Trials Registry Platform. There were no restrictions to language or year of publication. The date of the search was 5 May 2022.
Selection criteria: We included randomised controlled trials (RCTs) that compared pars plana vitrectomy and intravitreal injection of antibiotics versus intravitreal injection of antibiotics alone, for the immediate management of exogenous endophthalmitis.
Data collection and analysis: We used standard methods expected by Cochrane. Two review authors independently screened search results and extracted data. We considered the following outcomes: visual acuity improvement and change in visual acuity at three and six months; additional surgical procedures, including vitrectomy and cataract surgery, at any time during follow-up; quality of life and adverse effects. We assessed the certainty of the evidence using the GRADE approach. MAIN RESULTS: We identified a single RCT that met our inclusion criteria. The included RCT enrolled a total of 420 participants with clinical evidence of endophthalmitis, within six weeks of cataract surgery or secondary intraocular lens implantation. Participants were randomly assigned according to a 2 x 2 factorial design to either treatment with vitrectomy (VIT) or vitreous tap biopsy (TAP) and to treatment with or without systemic antibiotics. Twenty-four participants did not have a final follow-up: 12 died, five withdrew consent to be followed up, and seven were not willing to return for the visit. The study did not report visual acuity according to the review's predefined outcomes. At three months, 41% of all participants achieved 20/40 or better visual acuity and 69% had 20/100 or better acuity. The study authors reported that there was no statistically significant difference in visual acuity between treatment groups (very low-certainty evidence). There was low-certainty evidence of a similar requirement for additional surgical procedures (risk ratio RR 0.90, 95% confidence interval 0.66 to 1.21). Adverse effects included: VIT group: dislocated intraocular lens (n = 2), macular infarction (n = 1). TAP group: expulsive haemorrhage (n = 1). Quality of life and mean change in visual acuity were not reported. AUTHORS' CONCLUSIONS: We identified a single RCT (published 27 years ago) for the role of early vitrectomy in exogenous endophthalmitis, which suggests that there may be no difference between groups (VIT vs TAP) for visual acuity at three or nine months' follow-up. We are of the opinion that there is a clear need for more randomised studies comparing the role of primary vitrectomy in exogenous endophthalmitis. Moreover, since the original RCT study, there have been incremental changes in the surgical techniques with which vitrectomy is performed. Such advances are likely to influence the outcome of early vitrectomy in exogenous endophthalmitis.
Copyright © 2022 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
MMKM is a Consultant on a Scientific Advisory Board for Pixium Vision and joint‐principal investigator for an NIHR‐funded feasibility study investigating early vitrectomy in endophthalmitis. These are unpaid roles. MM: no conflicts of interest to declare. CB is a co‐applicant on a study investigating early vitrectomy in endophthalmitis. JWB has received payment for consultancy work from MeiraGTx Ltd and Novartis. Neither company has a direct interest in the subject of this review. He is also a joint‐principal investigator for an NIHR‐funded feasibility study investigating early vitrectomy in endophthalmitis; this is an unpaid role.
Figures



Update of
- doi: 10.1002/14651858.CD013760
Similar articles
-
Adjunctive steroid therapy versus antibiotics alone for acute endophthalmitis after intraocular procedure.Cochrane Database Syst Rev. 2017 Feb 22;2(2):CD012131. doi: 10.1002/14651858.CD012131.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2022 Jun 6;6:CD012131. doi: 10.1002/14651858.CD012131.pub3. PMID: 28225198 Free PMC article. Updated.
-
Adjunctive steroid therapy versus antibiotics alone for acute endophthalmitis after intraocular procedure.Cochrane Database Syst Rev. 2022 Jun 6;6(6):CD012131. doi: 10.1002/14651858.CD012131.pub3. Cochrane Database Syst Rev. 2022. PMID: 35665485 Free PMC article.
-
Perioperative antibiotics for prevention of acute endophthalmitis after cataract surgery.Cochrane Database Syst Rev. 2017 Feb 13;2(2):CD006364. doi: 10.1002/14651858.CD006364.pub3. Cochrane Database Syst Rev. 2017. PMID: 28192644 Free PMC article.
-
Surgical interventions for bilateral congenital cataract in children aged two years and under.Cochrane Database Syst Rev. 2022 Sep 15;9(9):CD003171. doi: 10.1002/14651858.CD003171.pub3. Cochrane Database Syst Rev. 2022. PMID: 36107778 Free PMC article.
-
Anti-vascular endothelial growth factor combined with intravitreal steroids for diabetic macular oedema.Cochrane Database Syst Rev. 2018 Apr 18;4(4):CD011599. doi: 10.1002/14651858.CD011599.pub2. Cochrane Database Syst Rev. 2018. PMID: 29669176 Free PMC article.
Cited by
-
Susceptibility of Ocular Surface Bacteria to Various Antibiotic Agents in a Romanian Ophthalmology Clinic.Diagnostics (Basel). 2023 Nov 9;13(22):3409. doi: 10.3390/diagnostics13223409. Diagnostics (Basel). 2023. PMID: 37998545 Free PMC article.
-
The diagnosis and treatment progress of infectious endophthalmitis.Eye (Lond). 2025 Feb;39(3):492-504. doi: 10.1038/s41433-024-03474-7. Epub 2024 Nov 30. Eye (Lond). 2025. PMID: 39616279 Review.
-
Timing of vitrectomy for treatment of endophthalmitis after intravitreal anti-VEGF injection: a systematic literature review of case reports and series.Ther Adv Ophthalmol. 2025 Jan 16;17:25158414241311064. doi: 10.1177/25158414241311064. eCollection 2025 Jan-Dec. Ther Adv Ophthalmol. 2025. PMID: 39831068 Free PMC article. Review.
-
Literature- and Experience-Based Consensus for Acute Post-operative Endophthalmitis and Endogenous Endophthalmitis in Taiwan.Ophthalmol Ther. 2024 Jan;13(1):1-19. doi: 10.1007/s40123-023-00835-5. Epub 2023 Nov 7. Ophthalmol Ther. 2024. PMID: 37934385 Free PMC article.
-
Post-Cataract Surgery Fungal Endophthalmitis: 6-Year Experience in Management and Outcomes at a Tertiary Eye Care Center.Clin Ophthalmol. 2024 Nov 4;18:3143-3151. doi: 10.2147/OPTH.S489090. eCollection 2024. Clin Ophthalmol. 2024. PMID: 39525871 Free PMC article.
References
References to studies included in this review
EVS Group 1995 {published data only}
-
- EVS Group. Results of the Endophthalmitis Vitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Endophthalmitis Vitrectomy Study Group. Archives of Ophthalmology 1995;113:1479-96. - PubMed
Additional references
AAO 2021
-
- American Academy of Ophthalmology. Cataract in the Adult Eye Preferred Practice Pattern; 2021. www.aao.org/preferred-practice-pattern/cataract-in-adult-eye-ppp-2021-in... . - PubMed
Astley 2016
Callegan 2007
Clarke 2018
-
- Clarke B, Williamson TH, Gini G, Gupta B. Management of bacterial postoperative endophthalmitis and the role of vitrectomy. Surveys in Ophthalmology 2018;63(5):677-93. - PubMed
Covidence [Computer program]
-
- Covidence. Version accessed 5 May 2022. Melbourne, Australia: Veritas Health Innovation. Available at covidence.org.
de Oliveira 2016
Du 2014
-
- Du DT, Wagoner A, Barone SB, Zinderman CE, Kelman JA, MaCurdy TE, et al. Incidence of endophthalmitis after corneal transplant or cataract surgery in a medicare population. Ophthalmology 2014;121(1):290-8. - PubMed
EMS working group 2021
Forster 1980
-
- Forster RK, Abbott RL, Gelender H. Management of infectious endophthalmitis. Ophthalmology 1980;87(4):313-9. - PubMed
Forster 1995
-
- Forster RK. The endophthalmitis vitrectomy study. Archives of Ophthalmology 1995;113(12):1555-7. - PubMed
Glanville 2006
GRADEpro GDT [Computer program]
-
- GRADEpro GDT. Version accessed 4 November 2021. Hamilton (ON): McMaster University (developed by Evidence Prime). Available at gradepro.org.
Higgins 2017
-
- Higgins JP, Altman DG, Sterne JA, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s). Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Kresloff 1998
-
- Kresloff MS, Castellarin AA, Zarbin MA. Endophthalmitis. Survery of Ophthalmology 1998;43(3):193-224. - PubMed
Kuhn 2005
-
- Kuhn F, Gini G. Ten years after... are findings of the Endophthalmitis Vitrectomy Study still relevant today? Graefe's Archive for Clinical and Experimental Ophthalmology 2005;243(12):1197–9. - PubMed
Maguire 2008
-
- Maguire JI. Postoperative endophthalmitis: optimal management and the role and timing of vitrectomy surgery. Eye 2008;22(10):1290-300. - PubMed
Relhan 2018
Review Manager 2020 [Computer program]
-
- Review Manager 5 (RevMan). Version 5.4. Copenhagen: The Cochrane Collaboration, 2020.
Scott 2011
-
- Scott IU, Flynn HW Jr, Acar N, Dev S, Shaikh S, Mittra RA, et al. Incidence of endophthalmitis after 20-gauge vs 23-gauge vs 25-gauge pars plana vitrectomy. Graefes Archive Clinical and Experimental Ophthalmology 2011;249(3):377-80. - PubMed
Stein 2009
Tan 2008
-
- Tan CS, Wong HK, Yang FP, Lee JJ. Outcome of 23-gauge sutureless transconjunctival vitrectomy for endophthalmitis. Eye 2008;22(1):150-1. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous