

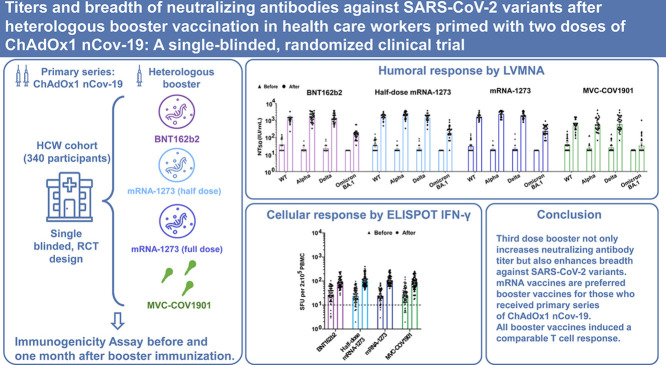
Titers and breadth of neutralizing antibodies against SARS-CoV-2 variants after heterologous booster vaccination in health care workers primed with two doses of ChAdOx1 nCov-19: A single-blinded, randomized clinical trial
- PMID: 36399969
- PMCID: PMC9651991
- DOI: 10.1016/j.jcv.2022.105328
Titers and breadth of neutralizing antibodies against SARS-CoV-2 variants after heterologous booster vaccination in health care workers primed with two doses of ChAdOx1 nCov-19: A single-blinded, randomized clinical trial
Abstract
Objectives: We conducted a single-blinded, randomized trial to evaluate the safety, reactogenicity, and immunogenicity of heterologous booster vaccination in health care workers (HCW) who had received two doses of ChAdOx1 nCov-19.
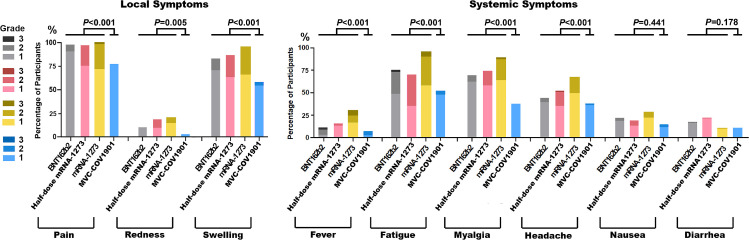
Methods: HCW who had at least 90 days after the second dose were enrolled to receive one of the four vaccines: BNT162b2 (30 μg), half-dose mRNA-1273 (50 μg), mRNA-1273 (100 μg), and MVC-COV1901 (15 μg). The primary outcomes were humoral and cellular immunogenicity and secondary outcomes assessed safety and reactogenicity at 28 days post-booster.
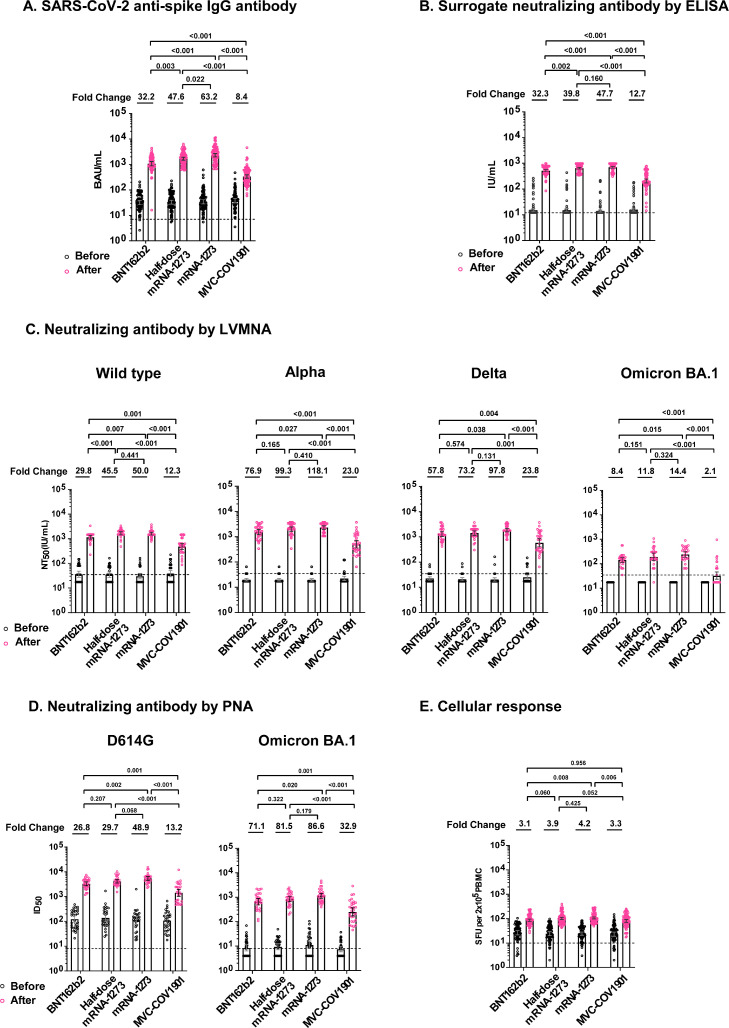
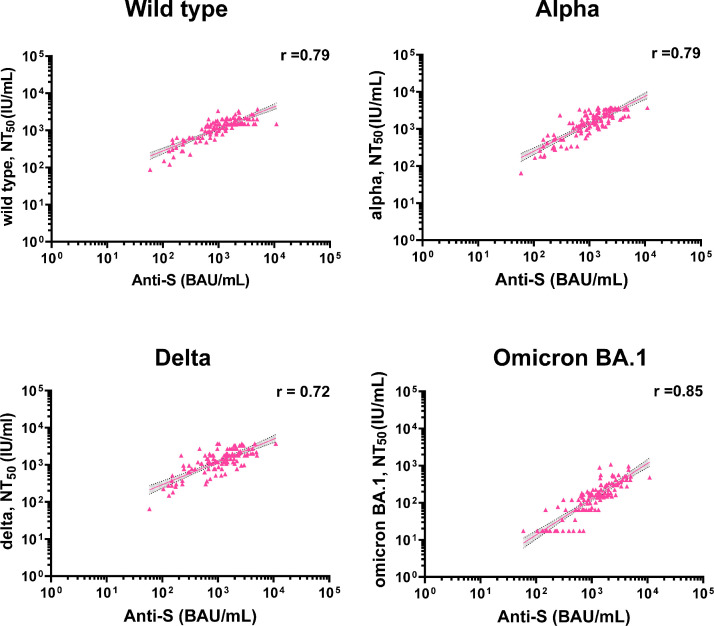
Results: MVC-COV1901 Three hundred and forty HCW were enrolled: 83 received BNT162b2 (2 excluded), 85 half-dose mRNA-1273, 85 mRNA-1273, and 85 MVC-COV1901. mRNA vaccines had more reactogenicity than protein vaccine. The fold-rise of anti-spike IgG geometric mean titer was 8.4 (95% CI 6.8-10.4) for MVC-COV1901, 32.2 (27.2-38.1) for BNT162b2, 47.6 (40.8-55.6) for half-dose mRNA-1273 and 63.2 (53.6-74.6) for mRNA-1273. The live virus microneutralization assays (LVMNA) against the wild type, alpha and delta variants were consistent with anti-spike IgG for all booster vaccines. The LVMNA in the four groups against omicron BA.1 variant were 6.4 to 13.5 times lower than those against the wild type. All booster vaccines induced a comparable T cell response.
Conclusions: Third dose booster not only increases neutralizing antibody titer but also enhances antibody breadth against SARS-CoV-2 variants. mRNA vaccines are preferred booster vaccines for those who received primary series of ChAdOx1 nCov-19.
Trial registration: ClinicalTrials.gov NCT05132855.
Keywords: COVID-19; Heterologous booster; Immunogenicity; Safety; Third dose; Vaccine.
Copyright © 2022 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no conflicts of interest.
Figures

References
-
- Doria-Rose N.A., Shen X., Schmidt S.D., O'Dell S., McDanal C., Feng W., et al. Booster of mRNA-1273 strengthens SARS-CoV-2 Omicron neutralization. medRxiv. 2021 doi: 10.1101/2021.12.15.21267805. 2021.12.15.21267805. - DOI
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
