

Low-level viraemia among people living with HIV in Nigeria: a retrospective longitudinal cohort study
- PMID: 36400087
- PMCID: PMC9711923
- DOI: 10.1016/S2214-109X(22)00413-2
Low-level viraemia among people living with HIV in Nigeria: a retrospective longitudinal cohort study
Abstract
Background: HIV transmission can occur with a viral load of at least 200 copies per mL of blood and low-level viraemia can lead to virological failure; the threshold level at which risk for virological failure is conferred is uncertain. To better understand low-level viraemia prevalence and outcomes, we analysed retrospective longitudinal data from a large cohort of people living with HIV on antiretroviral therapy (ART) in Nigeria.
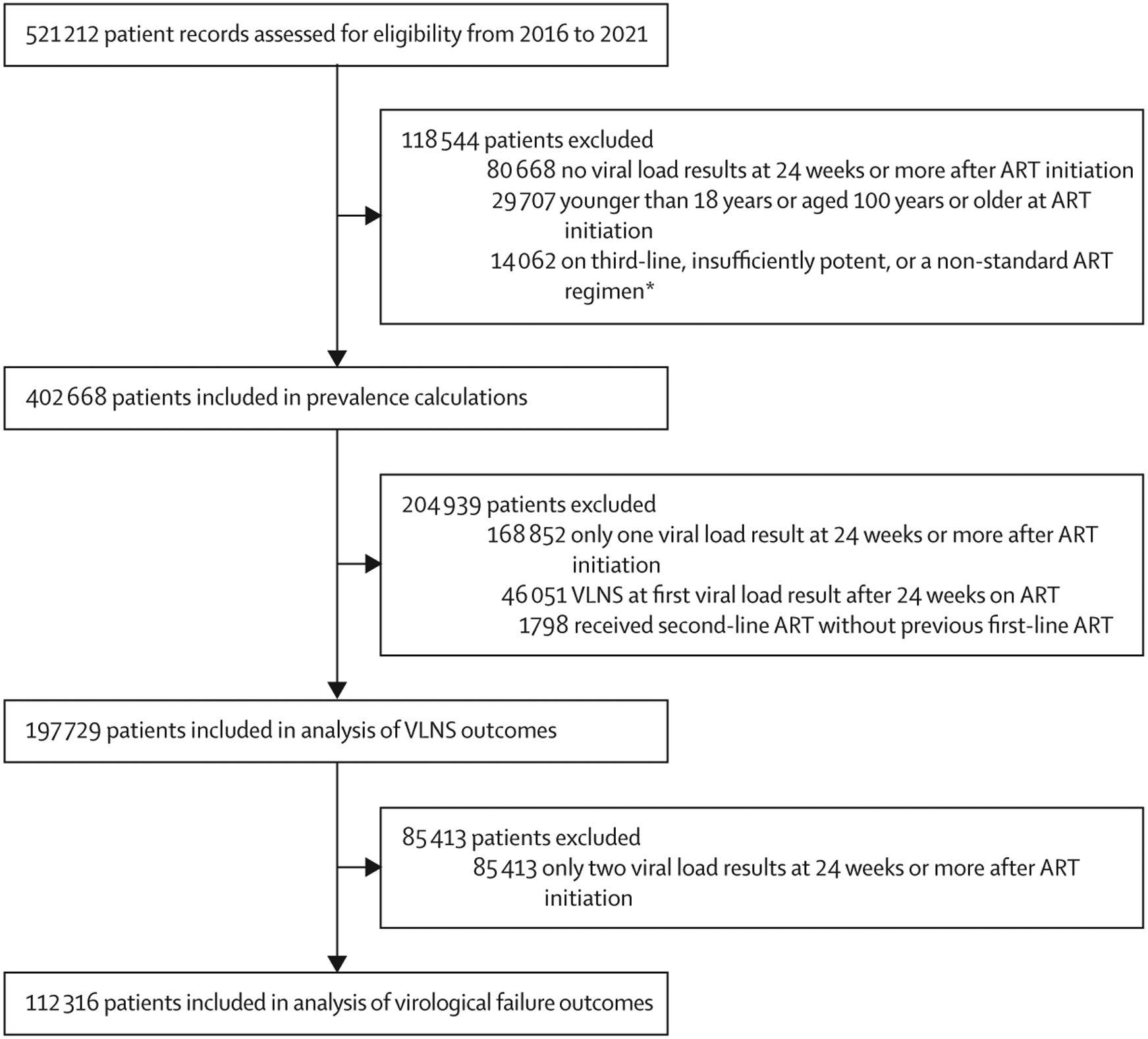
Methods: In this retrospective cohort study using previously collected longitudinal patient data, we estimated rates of virological suppression (≤50 copies per mL), low-level viraemia (51-999 copies per mL), virological non-suppression (≥1000 copies per mL), and virological failure (≥2 consecutive virological non-suppression results) among people living with HIV aged 18 years and older who initiated and received at least 24 weeks of ART at 1005 facilities in 18 Nigerian states. We analysed risk for low-level viraemia, virological non-suppression, and virological failure using log-binomial regression and mixed-effects logistic regression.
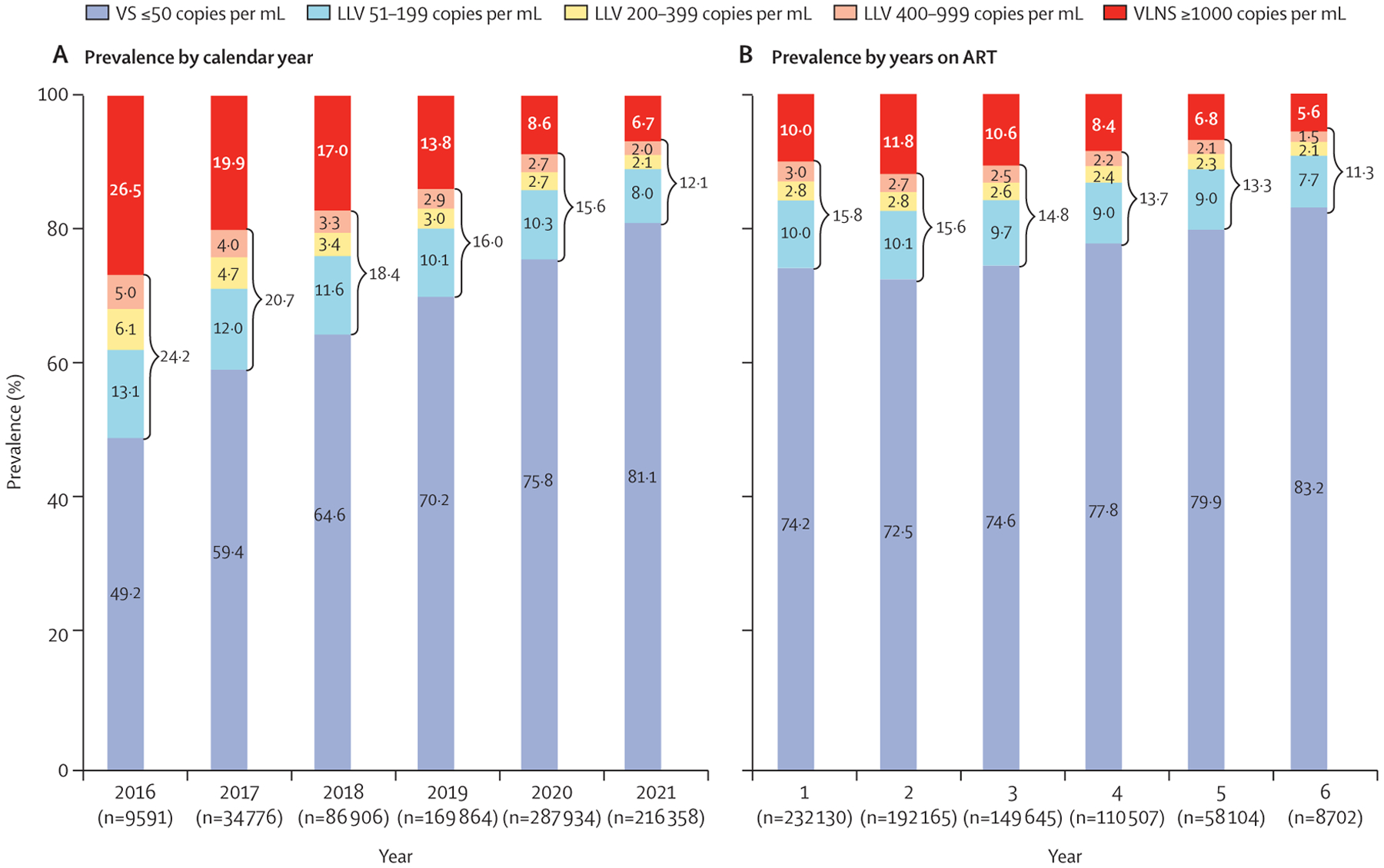
Findings: At first viral load for 402 668 patients during 2016-21, low-level viraemia was present in 64 480 (16·0%) individuals and virological non-suppression occurred in 46 051 (11·4%) individuals. Patients with low-level viraemia had increased risk of virological failure (adjusted relative risk 2·20, 95% CI 1·98-2·43; p<0·0001). Compared with patients with virological suppression, patients with low-level viraemia, even at 51-199 copies per mL, had increased odds of low-level viraemia and virological non-suppression at next viral load; patients on optimised ART (ie, integrase strand transfer inhibitors) had lower odds than those on non-integrase strand transfer inhibitors for the same low-level viraemia range (eg, viral load ≥1000 copies per mL following viral load 400-999 copies per mL, integrase strand transfer inhibitor: odds ratio 1·96, 95% CI 1·79-2·13; p<0·0001; non-integrase strand transfer inhibitor: 3·21, 2·90-3·55; p<0·0001).
Interpretation: Patients with low-level viraemia had increased risk of virological non-suppression and failure. Programmes should revise monitoring benchmarks and targets from less than 1000 copies per mL to less than 50 copies per mL to strengthen clinical outcomes and track progress to epidemic control.
Funding: None.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests We declare no competing interests.
Figures
Comment in
-
The virological consequences of low-level viraemia.Lancet Glob Health. 2022 Dec;10(12):e1699-e1700. doi: 10.1016/S2214-109X(22)00462-4. Lancet Glob Health. 2022. PMID: 36400076 No abstract available.
References
-
- Braitstein P, Brinkhof MW, Dabis F, et al. Mortality of HIV-1-infected patients in the first year of antiretroviral therapy: comparison between low-income and high-income countries. Lancet 2006; 367: 817–24. - PubMed
-
- Rodger AJ, Cambiano V, Bruun T, et al. Sexual activity without condoms and risk of HIV transmission in serodifferent couples when the HIV-positive partner is using suppressive antiretroviral therapy. JAMA 2016; 316: 171–81. - PubMed
-
- Vandenhende MA, Ingle S, May M, et al. Impact of low-level viremia on clinical and virological outcomes in treated HIV-1-infected patients. AIDS 2015; 29: 373–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
