

Perineural invasion and perineural spread in periocular squamous cell carcinoma
- PMID: 36400852
- PMCID: PMC10050156
- DOI: 10.1038/s41433-022-02306-w
Perineural invasion and perineural spread in periocular squamous cell carcinoma
Abstract
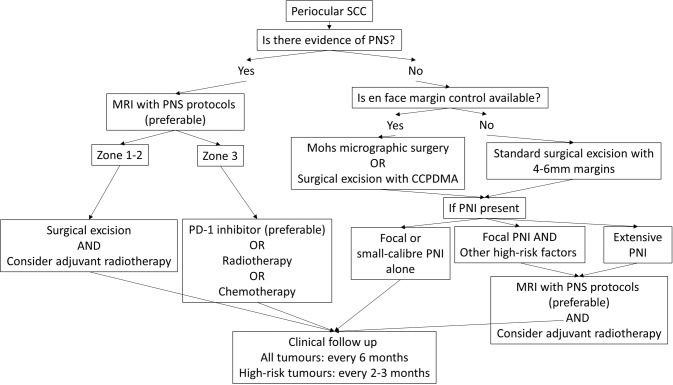
Perineural invasion (PNI) in cutaneous squamous cell carcinoma (SCC) of the periocular region is a prognostic marker of adverse tumour outcomes. PNI carries a well-established risk of tumour recurrence, regional metastasis and higher likelihood of mortality. This review will explore and stratify the risks conferred by histological PNI parameters. The radiological features of perineural spread (PNS) and the imaging sequences that delineate these findings will also be highlighted. Surgical excision with en face margin control is the preferred technique for achieving histological clearance. Adjuvant radiotherapy improves treatment outcomes in the setting of concomitant high-risk features. For locally advanced or metastatic cutaneous SCC, immunotherapy represents a novel treatment alternative. This review will provide an algorithm for the diagnosis and management of periocular SCC with PNI and PNS.
摘要: 眼周皮肤鳞状细胞癌 (SCC) 的周围神经浸润 (PNI) 是恶性肿瘤结局的预后标志。目前公认为PNI的出现具有肿瘤复发, 区域转移和高死亡率的风险。本综述将探讨并分层说明组织学PNI参数带来的风险。此外还重点介绍神经周围扩散 (PNS) 的放射学特征和描述这些结果的成像序列。手术切除联合en face控制边缘是实现组织学清除的首选技术。伴随高危特征的条件下, 辅助性放疗可改善治疗效果。对于局部晚期或转移性的 SCC, 免疫疗法代表了一种新型的治疗手段。本综述将为伴有PNI和PNS的SCC提供一个诊断和管理的算法。.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
What is the role of adjuvant radiotherapy in the treatment of cutaneous squamous cell carcinoma with perineural invasion?Cancer. 2007 Mar 15;109(6):1053-9. doi: 10.1002/cncr.22509. Cancer. 2007. PMID: 17279578 Review.
-
Management of periocular cutaneous squamous cell carcinoma with perineural invasion: a case series and literature review.Orbit. 2022 Feb;41(1):34-43. doi: 10.1080/01676830.2021.1893342. Epub 2021 Mar 4. Orbit. 2022. PMID: 33663321 Review.
-
Management Approaches for High-Risk Cutaneous Squamous Cell Carcinoma with Perineural Invasion: An Updated Review.Curr Treat Options Oncol. 2024 Sep;25(9):1184-1192. doi: 10.1007/s11864-024-01234-z. Epub 2024 Aug 5. Curr Treat Options Oncol. 2024. PMID: 39102167 Free PMC article. Review.
-
The status of perineural invasion predicts the outcomes of postoperative radiotherapy in locally advanced esophageal squamous cell carcinoma.Int J Clin Exp Pathol. 2015 Jun 1;8(6):6881-90. eCollection 2015. Int J Clin Exp Pathol. 2015. PMID: 26261575 Free PMC article.
-
Cutaneous squamous cell carcinoma with perineural invasion: report on eight cases and review of the literature.Dermatology. 2015;230(2):135-42. doi: 10.1159/000368771. Epub 2014 Dec 4. Dermatology. 2015. PMID: 25502983 Review.
Cited by
-
Intracranial extension of parotid adenoid cystic carcinoma presenting as trigeminal neuralgia: A case report.Radiol Case Rep. 2025 Mar 8;20(5):2346-2350. doi: 10.1016/j.radcr.2025.02.049. eCollection 2025 May. Radiol Case Rep. 2025. PMID: 40129804 Free PMC article.
-
Use of Supra-eyebrow Skin as a Frontalis Myocutaneous Flap to Reconstruct Temporal Skin Defect and Treat Facial Nerve Palsy: A Report of Two Cases.J Plast Reconstr Surg. 2024 Mar 1;3(3):124-127. doi: 10.53045/jprs.2023-0021. eCollection 2024 Jul 27. J Plast Reconstr Surg. 2024. PMID: 40103780 Free PMC article.
-
Head and neck nonmelanoma skin cancers: surgical management and debated issues.Curr Opin Otolaryngol Head Neck Surg. 2024 Apr 1;32(2):62-70. doi: 10.1097/MOO.0000000000000960. Epub 2024 Jan 3. Curr Opin Otolaryngol Head Neck Surg. 2024. PMID: 38193646 Free PMC article. Review.
-
Risk Factors for Orbital Invasion in Malignant Eyelid Tumors, Is Orbital Exenteration Still Necessary?J Clin Med. 2024 Jan 26;13(3):726. doi: 10.3390/jcm13030726. J Clin Med. 2024. PMID: 38337420 Free PMC article.
-
Normative data for dimensions of the frontal and infraorbital nerves.Eye (Lond). 2025 May;39(7):1390-1393. doi: 10.1038/s41433-025-03679-4. Epub 2025 Feb 7. Eye (Lond). 2025. PMID: 39920349 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
