

Effect of postextubation noninvasive ventilation with active humidification vs high-flow nasal cannula on reintubation in patients at very high risk for extubation failure: a randomized trial
- PMID: 36400984
- PMCID: PMC9676812
- DOI: 10.1007/s00134-022-06919-3
Effect of postextubation noninvasive ventilation with active humidification vs high-flow nasal cannula on reintubation in patients at very high risk for extubation failure: a randomized trial
Erratum in
-
Correction to: Effect of postextubation noninvasive ventilation with active humidification vs high-flow nasal cannula on reintubation in patients at very high risk for extubation failure: a randomized trial.Intensive Care Med. 2023 Mar;49(3):385. doi: 10.1007/s00134-023-06978-0. Intensive Care Med. 2023. PMID: 36705685 Free PMC article. No abstract available.
Abstract
Purpose: High-flow nasal cannula (HFNC) oxygen therapy was noninferior to noninvasive ventilation (NIV) for preventing reintubation in a heterogeneous population at high-risk for extubation failure. However, outcomes might differ in certain subgroups of patients. Thus, we aimed to determine whether NIV with active humidification is superior to HFNC in preventing reintubation in patients with ≥ 4 risk factors (very high risk for extubation failure).
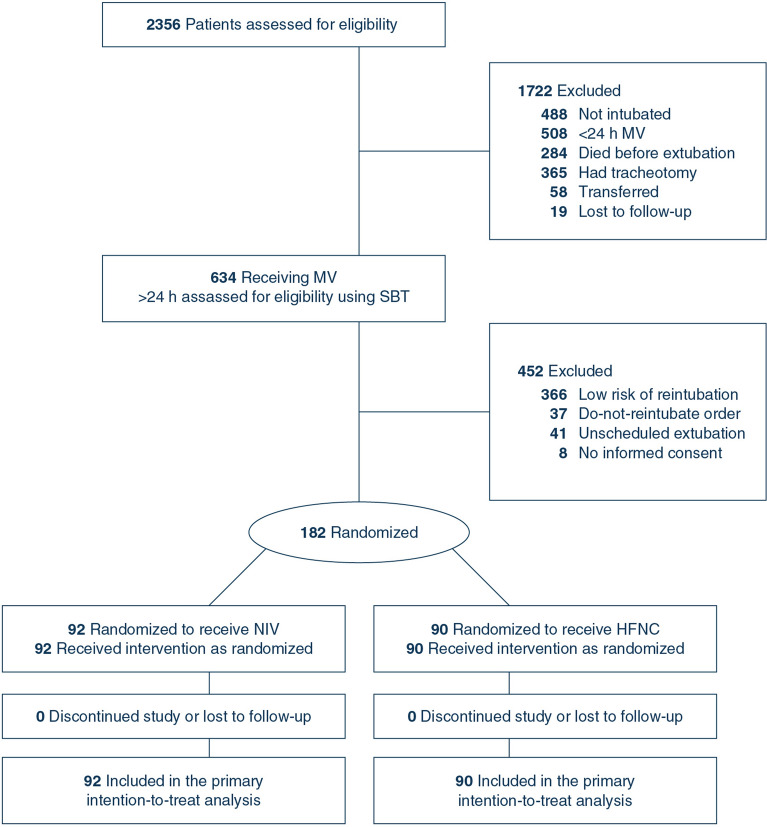
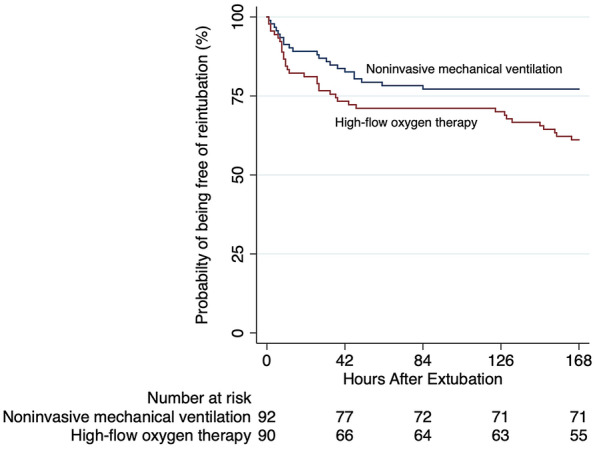
Methods: Randomized controlled trial in two intensive care units in Spain (June 2020‒June 2021). Patients ready for planned extubation with ≥ 4 of the following risk factors for reintubation were included: age > 65 years, Acute Physiology and Chronic Health Evaluation II score > 12 on extubation day, body mass index > 30, inadequate secretions management, difficult or prolonged weaning, ≥ 2 comorbidities, acute heart failure indicating mechanical ventilation, moderate-to-severe chronic obstructive pulmonary disease, airway patency problems, prolonged mechanical ventilation, or hypercapnia on finishing the spontaneous breathing trial. Patients were randomized to undergo NIV with active humidification or HFNC for 48 h after extubation. The primary outcome was reintubation rate within 7 days after extubation. Secondary outcomes included postextubation respiratory failure, respiratory infection, sepsis, multiorgan failure, length of stay, mortality, adverse events, and time to reintubation.
Results: Of 182 patients (mean age, 60 [standard deviation (SD), 15] years; 117 [64%] men), 92 received NIV and 90 HFNC. Reintubation was required in 21 (23.3%) patients receiving NIV vs 35 (38.8%) of those receiving HFNC (difference -15.5%; 95% confidence interval (CI) -28.3 to -1%). Hospital length of stay was lower in those patients treated with NIV (20 [12‒36.7] days vs 26.5 [15‒45] days, difference 6.5 [95%CI 0.5-21.1]). No additional differences in the other secondary outcomes were observed.
Conclusions: Among adult critically ill patients at very high-risk for extubation failure, NIV with active humidification was superior to HFNC for preventing reintubation.
Trial registration: ClinicalTrials.gov NCT04125342.
Keywords: Active humidification; High-flow nasal cannula; Noninvasive ventilation; Outcome; Reintubation; Weaning.
© 2022. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
All authors have completed and submitted the ICMJE Form for disclosure of potential conflicts of interest. GH reported travel expenses and personal fees from Fisher & Paykel Healthcare Ltd. OR reported a research grant from Hamilton Medical AG, speaker fees from Hamilton Medical AG, Fisher&Paykel Healthcare Ltd, Aerogen Ltd and Ambu, and non-financial research support from Timpel; all outside the submitted work.
Figures
Comment in
-
Post-extubation noninvasive ventilation vs high-flow nasal cannula on reintubation in patients at very high risk for extubation failure.Intensive Care Med. 2023 Mar;49(3):372-373. doi: 10.1007/s00134-022-06963-z. Epub 2023 Jan 4. Intensive Care Med. 2023. PMID: 36598547 No abstract available.
-
Postextubation ventilation strategy in preventing reintubation in patients at very high risk for extubation failure.Intensive Care Med. 2023 Mar;49(3):374-375. doi: 10.1007/s00134-023-06979-z. Epub 2023 Jan 16. Intensive Care Med. 2023. PMID: 36645447 No abstract available.
References
-
- Thille AW, Muller G, Gacouin A, et al. Effect of postextubation high-flow nasal oxygen with noninvasive ventilation vs high-flow nasal oxygen alone on reintubation among patients at high risk of extubation failure: a randomized clinical trial. JAMA. 2019;322(15):1465–1475. doi: 10.1001/jama.2019.14901. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
