

Impact of shifting from laparoscopic to robotic surgery during 600 minimally invasive pancreatic and liver resections
- PMID: 36401105
- PMCID: PMC10082117
- DOI: 10.1007/s00464-022-09735-4
Impact of shifting from laparoscopic to robotic surgery during 600 minimally invasive pancreatic and liver resections
Erratum in
-
Correction: Impact of shifting from laparoscopic to robotic surgery during 600 minimally invasive pancreatic and liver resections.Surg Endosc. 2023 Apr;37(4):3291-3292. doi: 10.1007/s00464-022-09848-w. Surg Endosc. 2023. PMID: 36575223 Free PMC article.
Abstract
Background: Many centers worldwide are shifting from laparoscopic to robotic minimally invasive hepato-pancreato-biliary resections (MIS-HPB) but large single center series assessing this process are lacking. We hypothesized that the introduction of robot-assisted surgery was safe and feasible in a high-volume center.
Methods: Single center, post-hoc assessment of prospectively collected data including all consecutive MIS-HPB resections (January 2010-February 2022). As of December 2018, all MIS pancreatoduodenectomy and liver resections were robot-assisted. All surgeons had participated in dedicated training programs for laparoscopic and robotic MIS-HPB. Primary outcomes were in-hospital/30-day mortality and Clavien-Dindo ≥ 3 complications.
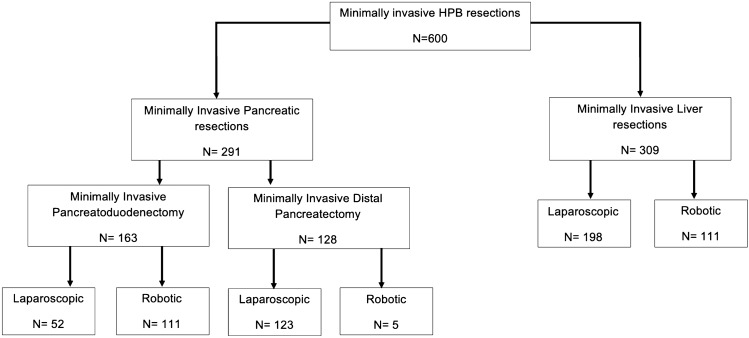
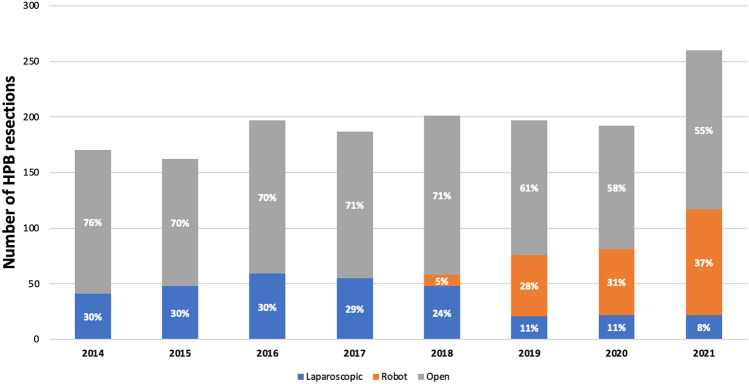
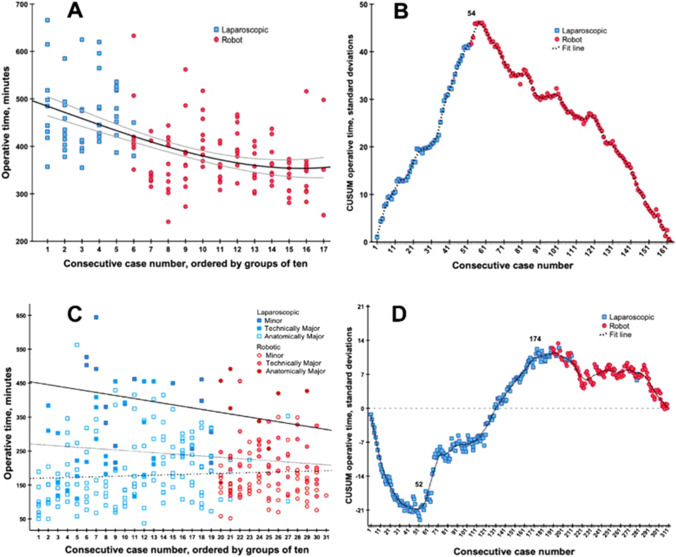
Results: Among 1875 pancreatic and liver resections, 600 (32%) were MIS-HPB resections. The overall rate of conversion was 4.3%, Clavien-Dindo ≥ 3 complications 25.7%, and in-hospital/30-day mortality 1.8% (n = 11). When comparing the period before and after the introduction of robotic MIS-HPB (Dec 2018), the overall use of MIS-HPB increased from 25.3 to 43.8% (P < 0.001) and blood loss decreased from 250 ml [IQR 100-500] to 150 ml [IQR 50-300] (P < 0.001). The 291 MIS pancreatic resections included 163 MIS pancreatoduodenectomies (52 laparoscopic, 111 robotic) with 4.3% conversion rate. The implementation of robotic pancreatoduodenectomy was associated with reduced operation time (450 vs 361 min; P < 0.001), reduced blood loss (350 vs 200 ml; P < 0.001), and a decreased rate of delayed gastric emptying (28.8% vs 9.9%; P = 0.009). The 309 MIS liver resections included 198 laparoscopic and 111 robotic procedures with a 3.6% conversion rate. The implementation of robotic liver resection was associated with less overall complications (24.7% vs 10.8%; P = 0.003) and shorter hospital stay (4 vs 3 days; P < 0.001).
Conclusion: The introduction of robotic surgery was associated with greater implementation of MIS-HPB in up to nearly half of all pancreatic and liver resections. Although mortality and major morbidity were not affected, robotic surgery was associated with improvements in some selected outcomes. Ultimately, randomized studies and high-quality registries should determine its added value.
Keywords: Distal pancreatectomy; Liver surgery; Minimally invasive; Pancreatoduodenectomy.
© 2022. The Author(s).
Conflict of interest statement
M.G. Besselink has received an Intuitive grant for the LEARNBOT European Robotic Pancreatoduodenectomy training program, the DIPLOMA-2 trial and the E-MIPS quality registry. A Medtronic grant for the investigator-initiated DIPLOMA trial. An Ethicon grant for the PANDORINA trial and the E-MIPS quality registry. A.M.L.H. Emmen, B. Görgec, M.J.W. Zwart, F. Daams, J. Erdmann, S. Festen, D.J. Gouma, T.M. van Gulik, J. van Hilst, G. Kazemier, S. Lof, S.I. Sussenbach, P.J. Tanis, B.M. Zonderhuis, O.R. Busch, R.J. Swijnenburg have no conflict of interest or financial ties to disclose.
Figures
Similar articles
-
Minimally Invasive Hepatopancreatobiliary Surgery at a Large Regional Health System: Assessing the Safety of Program Expansion.Am Surg. 2024 Jan;90(1):85-91. doi: 10.1177/00031348231192073. Epub 2023 Aug 14. Am Surg. 2024. PMID: 37578387
-
[Robot-Assisted Upper Gastrointestinal and Hepato-Pancreato-Biliary Surgery: Implementation Using a Stepwise Approach and Analyses of the First 100 Surgical Procedures].Zentralbl Chir. 2020 Jun;145(3):234-245. doi: 10.1055/a-1135-9277. Epub 2020 Jun 4. Zentralbl Chir. 2020. PMID: 32498109 German.
-
Implementation of a robotic hepato-pancreato-biliary surgery program: a swedish referral center's experience.J Robot Surg. 2025 Mar 6;19(1):101. doi: 10.1007/s11701-025-02241-4. J Robot Surg. 2025. PMID: 40047977
-
Robotic hepatectomy and biliary reconstruction for perihilar cholangiocarcinoma: a pioneer western case series.Updates Surg. 2021 Jun;73(3):999-1006. doi: 10.1007/s13304-021-01041-3. Epub 2021 Apr 16. Updates Surg. 2021. PMID: 33861401 Free PMC article. Review.
-
Minimally invasive hepatopancreatic and biliary surgery in children: a large centre experience and review of the literature.HPB (Oxford). 2022 Jun;24(6):857-867. doi: 10.1016/j.hpb.2021.10.013. Epub 2021 Oct 31. HPB (Oxford). 2022. PMID: 34810094 Review.
Cited by
-
The Brescia internationally validated European guidelines on minimally invasive liver surgery.Br J Surg. 2025 May 31;112(6):znaf113. doi: 10.1093/bjs/znaf113. Br J Surg. 2025. PMID: 40568914 Free PMC article. No abstract available.
-
Robotic liver parenchymal transection techniques: a comprehensive overview and classification.J Robot Surg. 2024 Dec 30;19(1):36. doi: 10.1007/s11701-024-02200-5. J Robot Surg. 2024. PMID: 39738738 Review.
-
Robotic vs laparoscopic approaches of pancreatic resection: a systematic review and meta-analysis.J Robot Surg. 2025 Jun 16;19(1):295. doi: 10.1007/s11701-025-02446-7. J Robot Surg. 2025. PMID: 40522553 Review.
-
Perioperative outcomes of robotic vs laparoscopic pancreatoduodenectomy: a meta-analysis and trial sequential analysis.Surg Endosc. 2025 Mar;39(3):1462-1472. doi: 10.1007/s00464-024-11515-1. Epub 2025 Jan 29. Surg Endosc. 2025. PMID: 39880981
-
Robotic hepaticojejunostomy training in novices using robotic simulation and dry-lab suturing (ROSIM): randomized controlled crossover trial.Surg Endosc. 2024 Sep;38(9):4906-4915. doi: 10.1007/s00464-024-10914-8. Epub 2024 Jul 3. Surg Endosc. 2024. PMID: 38958718 Free PMC article. Clinical Trial.
References
-
- Cuschieri A. Laparoscopic surgery of the pancreas. J R Coll Surg Edinb. 1994;39:178–184. - PubMed
-
- van Hilst J, De Rooij T, Bosscha K, et al. Laparoscopic versus open pancreatoduodenectomy for pancreatic or periampullary tumours (LEOPARD-2): a multicentre, patient-blinded, randomised controlled phase 2/3 trial. Lancet Gastroenterol. Hepatol. 2019;4:199–207. doi: 10.1016/S2468-1253(19)30004-4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
