

A mixed-methods feasibility study of a new digital health support package for people after stroke: the Recovery-focused Community support to Avoid readmissions and improve Participation after Stroke (ReCAPS) intervention
- PMID: 36401336
- PMCID: PMC9675218
- DOI: 10.1186/s40814-022-01197-8
A mixed-methods feasibility study of a new digital health support package for people after stroke: the Recovery-focused Community support to Avoid readmissions and improve Participation after Stroke (ReCAPS) intervention
Abstract
Background: Evidence for digital health programmes to support people living with stroke is growing. We assessed the feasibility of a protocol and procedures for the Recovery-focused Community support to Avoid readmissions and improve Participation after Stroke (ReCAPS) trial.
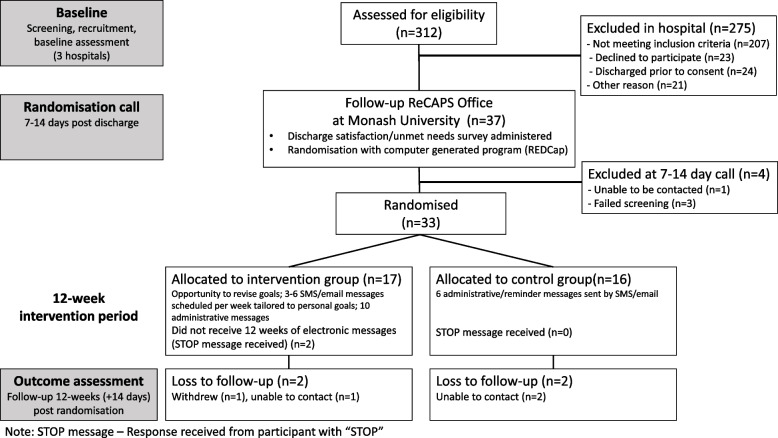
Methods: We conducted a mixed-method feasibility study. Participants with acute stroke were recruited from three hospitals (Melbourne, Australia). Eligibility: Adults with stroke discharged from hospital to home within 10 days, modified Rankin Score 0-4 and prior use of Short Message System (SMS)/email. While in hospital, recruited participants contributed to structured person-centred goal setting and completed baseline surveys including self-management skills and health-related quality of life. Participants were randomised 7-14 days after discharge via REDCap® (1:1 allocation). Following randomisation, the intervention group received a 12-week programme of personalised electronic support messages (average 66 messages sent by SMS or email) aligned with their goals. The control group received six electronic administrative messages. Feasibility outcomes included the following: number of patients screened and recruited, study retainment, completion of outcome measures and acceptability of the ReCAPS intervention and trial procedures (e.g. participant satisfaction survey, clinician interviews). Protocol fidelity outcomes included number of goals developed (and quality), electronic messages delivered, stop messages received and engagement with messages. We undertook inductive thematic analysis of interview/open-text survey data and descriptive analysis of closed survey questions.
Results: Between November 2018 and October 2019, 312 patients were screened; 37/105 (35%) eligible patients provided consent (mean age 61 years; 32% female); 33 were randomised (17 to intervention). Overall, 29 (88%) participants completed the12-week outcome assessments with 12 (41%) completed assessments in the allocated timeframe and 16 also completing the satisfaction survey (intervention=10). Overall, trial participants felt that the study was worthwhile and most would recommend it to others. Six clinicians participated in one of three focus group interviews; while they reported that the trial and the process of goal setting were acceptable, they raised concerns regarding the additional time required to personalise goals.
Conclusion: The study protocol and procedures were feasible with acceptable retention of participants. Consent and goal personalisation procedures should be centralised for the phase III trial to reduce the burden on hospital clinicians.
Trial registration: Australian New Zealand Clinical Trials Registry, ACTRN12618001468213 (date 31/08/2018); Universal Trial Number: U1111-1206-7237.
Keywords: Digital health; Feasibility study; Healthcare technology; Stroke; eHealth.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- National Stroke Foundation . Walk in our shoes. Stroke survivors and carers report on support after stroke. Melbourne: National Stroke Foundation; 2007.
LinkOut - more resources
Full Text Sources
