

Impact of tumor size on the difficulty of laparoscopic left lateral sectionectomies
- PMID: 36401813
- PMCID: PMC10195918
- DOI: 10.1002/jhbp.1279
Impact of tumor size on the difficulty of laparoscopic left lateral sectionectomies
Abstract
Background: Tumor size (TS) represents a critical parameter in the risk assessment of laparoscopic liver resections (LLR). Moreover, TS has been rarely related to the extent of liver resection. The aim of this study was to study the relationship between tumor size and difficulty of laparoscopic left lateral sectionectomy (L-LLS).
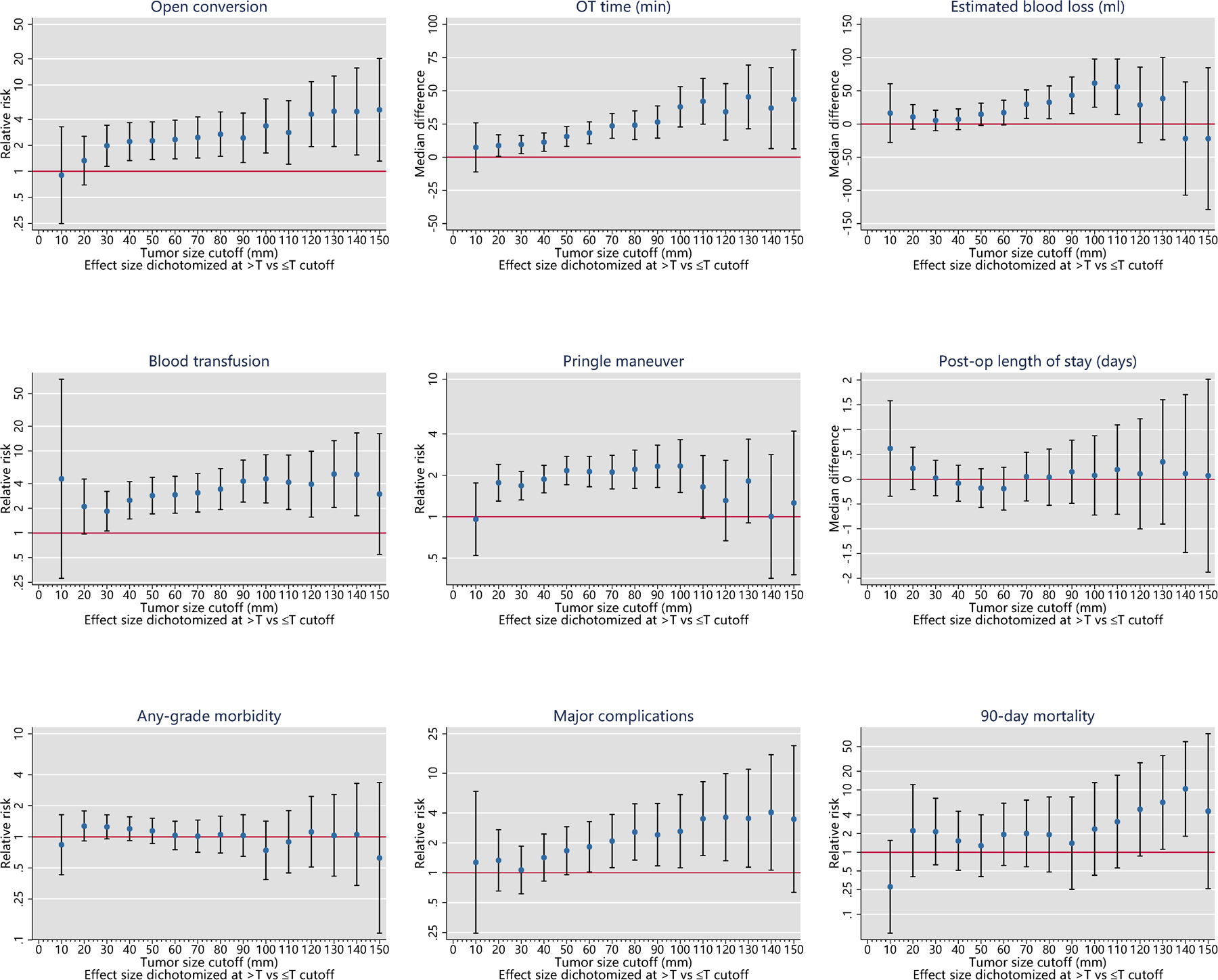
Methods: The impact of TS cutoffs was investigated by stratifying tumor size at each 10 mm-interval. The optimal cutoffs were chosen taking into consideration the number of endpoints which show a statistically significant split around the cut-points of interest and the magnitude of relative risk after correction for multiple risk factors.
Results: A total of 1910 L-LLS were included. Overall, open conversion and intraoperative blood transfusion were 3.1 and 3.3%, respectively. The major morbidity rate was 2.7% and 90-days mortality 0.6%. Three optimal TS cutoffs were identified: 40-, 70-, and 100-mm. All the selected cutoffs showed a significant discriminative power for the prediction of open conversion, operative time, blood transfusion and need of Pringle maneuver. Moreover, 70- and 100-mm cutoffs were both discriminative for estimated blood loss and major complications. A stepwise increase in rates of open conversion rate (Z = 3.90, P < .001), operative time (Z = 3.84, P < .001), blood loss (Z = 6.50, P < .001), intraoperative blood transfusion rate (Z = 5.15, P < .001), Pringle maneuver use (Z = 6.48, P < .001), major morbidity(Z = 2.17, P = .030) and 30-days readmission (Z = 1.99, P = .047) was registered as the size increased.
Conclusion: L-LLS for tumors of increasing size was associated with poorer intraoperative and early postoperative outcomes suggesting increasing difficulty of the procedure. We determined three optimal TS cutoffs (40-, 70- and 100-mm) to accurately stratify surgical difficulty after L-LLS.
Keywords: difficulty; laparoscopic hepatectomy; laparoscopic liver; left lateral sectionectomy; size.
© 2022 Japanese Society of Hepato-Biliary-Pancreatic Surgery.
Conflict of interest statement
Dr Goh BK has received travel grants and honorarium from Johnson and Johnson, Olympus and Transmedic the local distributor for the Da Vinci Robot.
Dr Marino MV is a consultant for CAVA robotics LLC.
Johann Pratschke reports a research grant from Intuitive Surgical Deutschland GmbH and personal fees or non-financial support from Johnson & Johnson, Medtronic, AFS Medical, Astellas, CHG Meridian, Chiesi, Falk Foundation, La Fource Group, Merck, Neovii, NOGGO, pharma- consult Peterson, and Promedicis.
Moritz Schmelzle reports personal fees or other support outside of the submitted work from Merck, Bayer, ERBE, Amgen, Johnson & Johnson, Takeda, Olympus, Medtronic, Intuitive.
Asmund Fretland reports receiving speaker fees from Bayer.
Fernando Rotellar reports speaker fees and support outside the submitted work from Integra, Medtronic, Olympus, Corza, Sirtex and Johnson & Johnson.
References
-
- Wakabayashi G, Cherqui D, Geller DA et al.; Recommendations for laparoscopic liver resection: a report from the second international consensus conference held in Morioka. Ann Surg. 2015. Apr;261(4):619–29. - PubMed
-
- Halls MC, Berardi G, Cipriani F et al.; Development and validation of a difficulty score to pre- dict intraoperative complications during laparoscopic liver resection. Br J Surg. 2018. Aug;105(9):1182–1191. - PubMed
-
- Kabir T, Syn N, Koh YX, Teo JY, Chung AY, Chan CY, Goh BKP. Impact of tumor size on the difficulty of minimally invasive liver resection. Eur J Surg Oncol. 2022. Jan;48(1):169–176. - PubMed
-
- Russolillo N, Casella M, Langella S, Lo Tesoriere R, Ossola P, Ferrero A. Correlation between anthropometric data and preparatory maneuvers difficulties during laparoscopic right liver resec- tions: a single center prospective study. Surg Endosc. 2022. Feb 24. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
