

In-hospital and 6-month outcomes in patients with COVID-19 supported with extracorporeal membrane oxygenation (EuroECMO-COVID): a multicentre, prospective observational study
- PMID: 36402148
- PMCID: PMC9671669
- DOI: 10.1016/S2213-2600(22)00403-9
In-hospital and 6-month outcomes in patients with COVID-19 supported with extracorporeal membrane oxygenation (EuroECMO-COVID): a multicentre, prospective observational study
Abstract
Background: Extracorporeal membrane oxygenation (ECMO) has been widely used in patients with COVID-19, but uncertainty remains about the determinants of in-hospital mortality and data on post-discharge outcomes are scarce. The aims of this study were to investigate the variables associated with in-hospital outcomes in patients who received ECMO during the first wave of COVID-19 and to describe the status of patients 6 months after ECMO initiation.
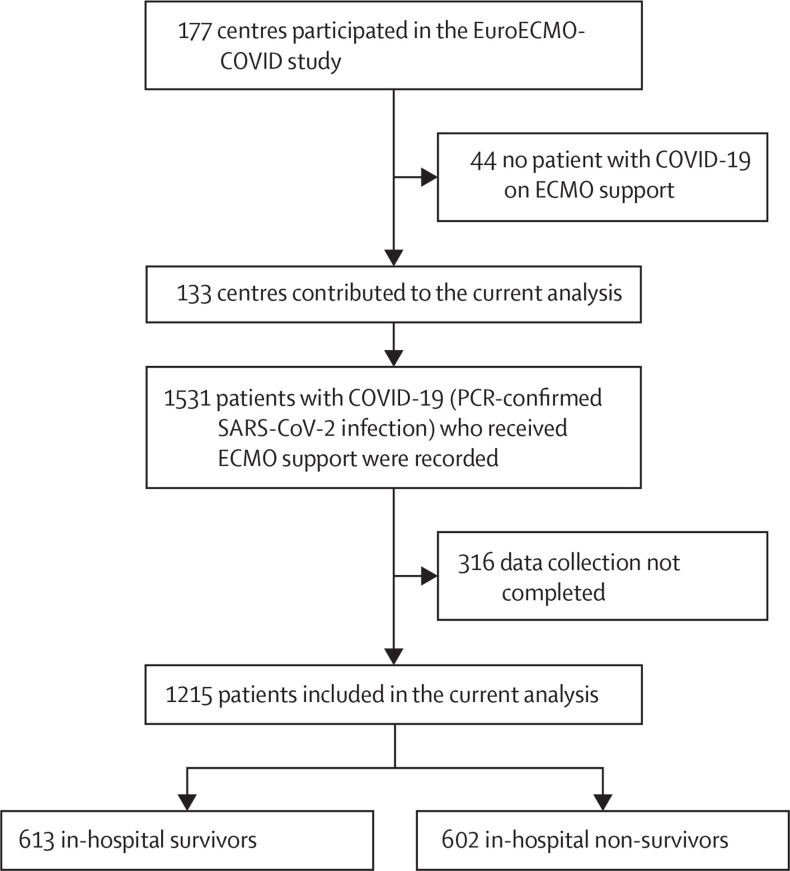
Methods: EuroECMO-COVID is a prospective, multicentre, observational study developed by the European Extracorporeal Life Support Organization. This study was based on data from patients aged 16 years or older who received ECMO support for refractory COVID-19 during the first wave of the pandemic-from March 1 to Sept 13, 2020-at 133 centres in 21 countries. In-hospital mortality and mortality 6 months after ECMO initiation were the primary outcomes. Mixed-Cox proportional hazards models were used to investigate associations between patient and management-related variables (eg, patient demographics, comorbidities, pre-ECMO status, and ECMO characteristics and complications) and in-hospital deaths. Survival status at 6 months was established through patient contact or institutional charts review. This study is registered with ClinicalTrials.gov, NCT04366921, and is ongoing.
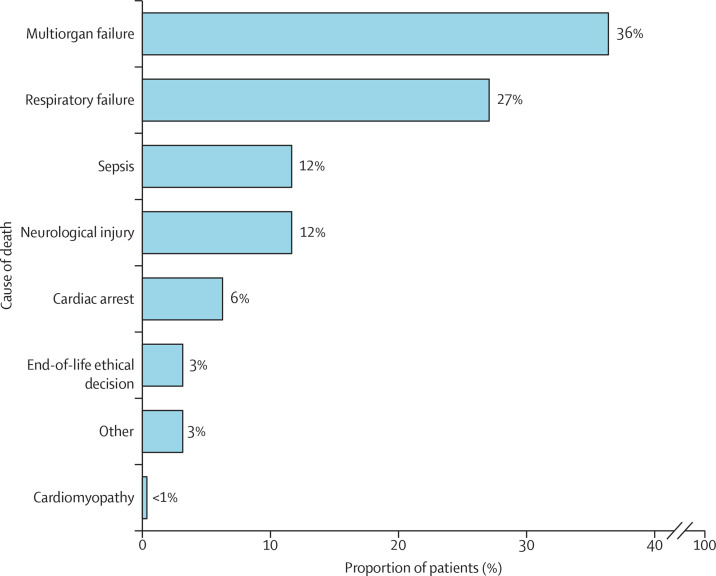
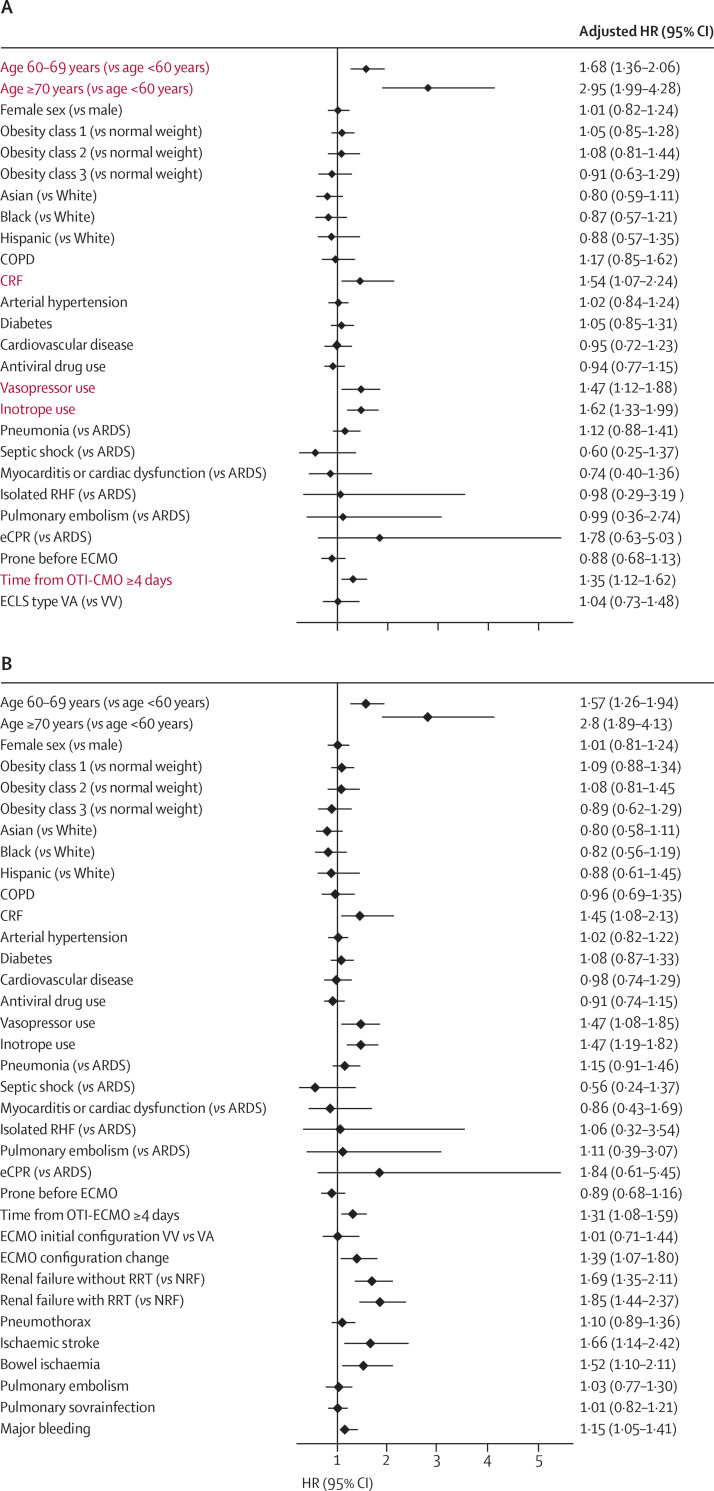
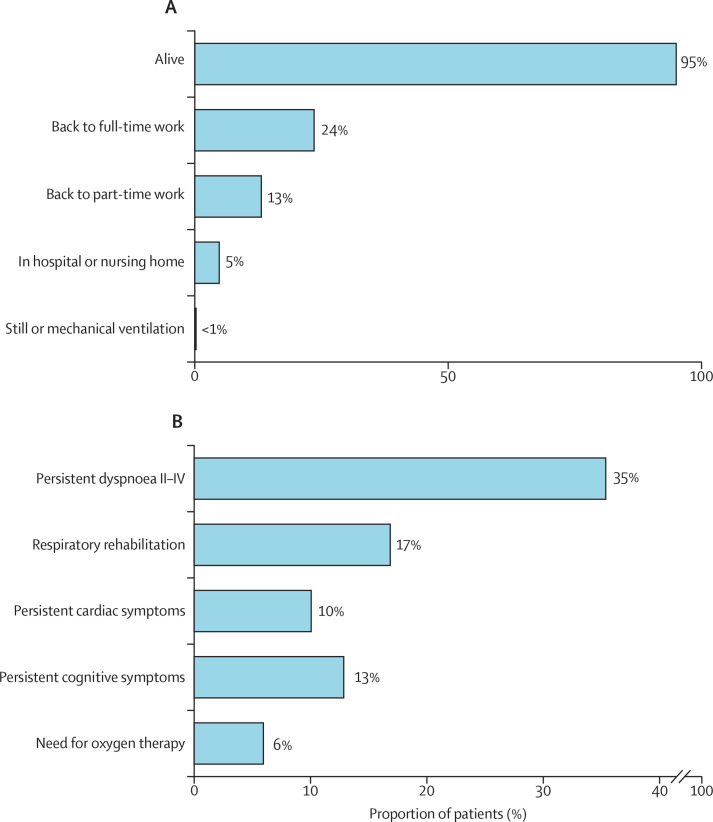
Findings: Between March 1 and Sept 13, 2020, 1215 patients (942 [78%] men and 267 [22%] women; median age 53 years [IQR 46-60]) were included in the study. Median ECMO duration was 15 days (IQR 8-27). 602 (50%) of 1215 patients died in hospital, and 852 (74%) patients had at least one complication. Multiorgan failure was the leading cause of death (192 [36%] of 528 patients who died with available data). In mixed-Cox analyses, age of 60 years or older, use of inotropes and vasopressors before ECMO initiation, chronic renal failure, and time from intubation to ECMO initiation of 4 days or more were associated with higher in-hospital mortality. 613 patients did not die in hospital, and 547 (95%) of 577 patients for whom data were available were alive at 6 months. 102 (24%) of 431 patients had returned to full-time work at 6 months, and 57 (13%) of 428 patients had returned to part-time work. At 6 months, respiratory rehabilitation was required in 88 (17%) of 522 patients with available data, and the most common residual symptoms included dyspnoea (185 [35%] of 523 patients) and cardiac (52 [10%] of 514 patients) or neurocognitive (66 [13%] of 512 patients) symptoms.
Interpretation: Patient's age, timing of cannulation (<4 days vs ≥4 days from intubation), and use of inotropes and vasopressors are essential factors to consider when analysing the outcomes of patients receiving ECMO for COVID-19. Despite post-discharge survival being favourable, persisting long-term symptoms suggest that dedicated post-ECMO follow-up programmes are required.
Funding: None.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests RL and JBe are past chairmen of the European Extracorporeal Life Support Organization (ELSO) Steering Committee. NB is the current chairman of the European ELSO Steering Committee. MVA, NB, JBe, MB, MDM, TM, JR, and JS are European ELSO Steering Committee members. RL reports personal fees from Abiomed and Xenios and honoraria payed institution from Medtronic, LivaNova, Getinge and Eurosets, unrelated to the submitted works. FST is advisory member for Eurosets unrelated to the submitted work. DW is proctor for Abbott and scientific advisor for Fresenius. NB is advisory board for ALung. JR reports lecture and advisory fees from Medtronic and Werfen outside the submitted work. PS reports advisory fees from Getinge but not related to the submitted work. AV received consultant fees from Inspira Technologies. MB is an advisory member for Eurosets, congress speaker for Hamilton Medical, and course speaker for Estor, all unrelated to the submitted work. LMB is advisory board for Eurosets and Xenios and is board member of EuroELSO Enterprise, unrelated to the present work. JBe reports consultancy and lecture fees from Abiomed and Getinge and is advisory board member of AstraZeneca and Boehringer Ingelheim. SL is advisory member of Inspira Technologies, unrelated to the present work. All other authors declare no competing interests.
Figures
Comment in
-
VV-ECMO in severe COVID-19: multidimensional perspectives on the use of a complex treatment.Lancet Respir Med. 2023 Feb;11(2):113-115. doi: 10.1016/S2213-2600(22)00487-8. Epub 2023 Jan 11. Lancet Respir Med. 2023. PMID: 36640787 Free PMC article. No abstract available.
-
Determinants of long-term outcomes in patients with COVID-19 supported with ECMO - Authors' reply.Lancet Respir Med. 2023 May;11(5):e42. doi: 10.1016/S2213-2600(23)00134-0. Epub 2023 Apr 5. Lancet Respir Med. 2023. PMID: 37030307 Free PMC article. No abstract available.
-
Determinants of long-term outcomes in patients with COVID-19 supported with ECMO.Lancet Respir Med. 2023 May;11(5):e41. doi: 10.1016/S2213-2600(23)00010-3. Epub 2023 Apr 5. Lancet Respir Med. 2023. PMID: 37030309 Free PMC article. No abstract available.
References
-
- WHO COVID-19 Dashboard. 2021. https://covid19.who.int/ (accessed Nov 4, 2022).
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
