

Longitudinal changes in fibrosis markers are associated with risk of cirrhosis and hepatocellular carcinoma in non-alcoholic fatty liver disease
- PMID: 36402450
- PMCID: PMC10661838
- DOI: 10.1016/j.jhep.2022.10.035
Longitudinal changes in fibrosis markers are associated with risk of cirrhosis and hepatocellular carcinoma in non-alcoholic fatty liver disease
Abstract
Background & aims: Currently, there is no consistent information on the course of fibrosis-4 (FIB-4) score changes in non-alcoholic fatty liver disease (NAFLD) or their association with subsequent risk of cirrhosis and/or hepatocellular carcinoma (HCC). Thus, we aimed to evaluate the association between longitudinal changes in FIB-4 and subsequent risk of HCC and a composite endpoint of cirrhosis and HCC in patients with NAFLD.
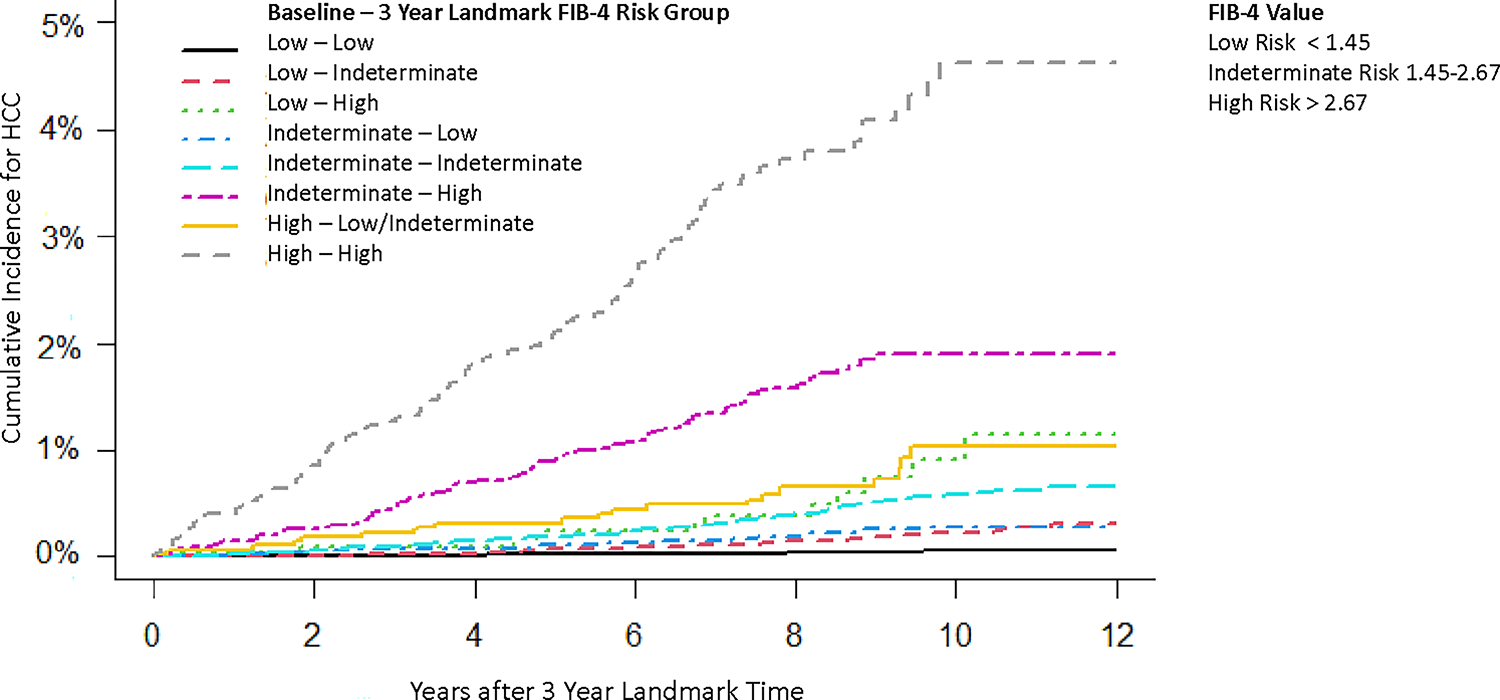
Methods: We conducted a retrospective cohort study of patients with NAFLD seen in 130 Veterans Administration hospitals between 1/1/2004-12/31/2008, with follow-up through to 12/31/2018. We calculated FIB-4 longitudinally and categorized patients based on risk of advanced fibrosis (low-risk FIB-4 <1.45, indeterminate-risk FIB-4 1.45-2.67, and high-risk FIB-4 >2.67). We used landmark Fine-Gray competing risks models to determine the effects of change in FIB-4 between NAFLD diagnosis date and 3-year landmark time on the subsequent risk of HCC and a composite endpoint.
Results: Among the 202,319 patients with NAFLD in the 3-year landmark analysis, 473 progressed to HCC at an incidence rate of 0.28 per 1,000 person years (PY) (95% CI 0.26-0.30). The incidence rate of the composite endpoint was 1.31 per 1,000 PY (95% CI 1.25-1.37). At baseline, 74.7%, 21.4%, and 3.8% of patients had a low, indeterminate, and high FIB-4, respectively. Compared to patients who were at stable low FIB-4 at both time points, the risk of HCC and that of the composite endpoint was higher for all other subgroups with the highest risk in patients with persistently high FIB-4 (HCC adjusted sub-distribution hazard ratio 57.7, 95% CI 40.5-82.2 and composite endpoint hazard ratio 28.6, 95% CI 24.6-33.2).
Conclusion: Longitudinal changes in FIB-4 were strongly associated with progression to cirrhosis and HCC.
Impact and implications: Tools to stratify the risk of HCC development in patients with NAFLD are currently lacking. The fibrosis-4 (FIB-4) score is a widely available non-invasive test for liver fibrosis, a primary determinant of the development of cirrhosis and HCC. In a large retrospective cohort of patients with NAFLD, we found that serial changes in FIB-4 over time were strongly associated with progression to cirrhosis and HCC. Integrating serial measurements of non-invasive tests for fibrosis into the care pathway for patients with NAFLD could help tailor HCC risk prevention.
Keywords: HCC; NAFLD; Risk stratification; fibrosis; non-invasive fibrosis markers.
Copyright © 2022. Published by Elsevier B.V.
Conflict of interest statement
Conflict of interest
Dr. Kanwal and Kramer are investigators at IQuESt. The authors have no other relevant financial disclosures or conflicts of interest.
Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
Comment in
-
Longitudinal changes in fatty liver index are associated with risk of hepatocellular carcinoma: A nationwide cohort study in Korea.J Hepatol. 2024 May;80(5):e216-e218. doi: 10.1016/j.jhep.2023.09.036. Epub 2023 Oct 11. J Hepatol. 2024. PMID: 37827474 No abstract available.
-
Surveillance for hepatocellular carcinoma in non-alcoholic fatty liver disease patients: towards personalized risk stratification.Hepatobiliary Surg Nutr. 2023 Dec 1;12(6):927-929. doi: 10.21037/hbsn-23-501. Epub 2023 Nov 8. Hepatobiliary Surg Nutr. 2023. PMID: 38115941 Free PMC article. No abstract available.
-
Clinical utility of non-invasive tests to predict clinical outcomes in non-alcoholic fatty liver disease.Hepatobiliary Surg Nutr. 2023 Dec 1;12(6):916-918. doi: 10.21037/hbsn-23-460. Epub 2023 Nov 1. Hepatobiliary Surg Nutr. 2023. PMID: 38115945 Free PMC article. No abstract available.
References
-
- Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016; 64:73–84. - PubMed
-
- Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol 2018;15:11–20. - PubMed
-
- Williams CD, Stengel J, Asike MI, Torres DM, Shaw J, Contreras M, et al. Prevalence of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among a largely middle-aged population utilizing ultrasound and liver biopsy: a prospective study. Gastroenterology 2011;140:124–131. - PubMed
-
- Kabbany MN, Conjeevaram Selvakumar PK, Watt K, Lopez R, Akras Z, Zein N, et al. Prevalence of nonalcoholic steatohepatitis-associated cirrhosis in the United States: an analysis of national Health and nutrition examination survey data. Am J Gastroenterol 2017;112:581–587. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
