

Increased biventricular hemodynamic forces in precapillary pulmonary hypertension
- PMID: 36402861
- PMCID: PMC9675772
- DOI: 10.1038/s41598-022-24267-6
Increased biventricular hemodynamic forces in precapillary pulmonary hypertension
Abstract
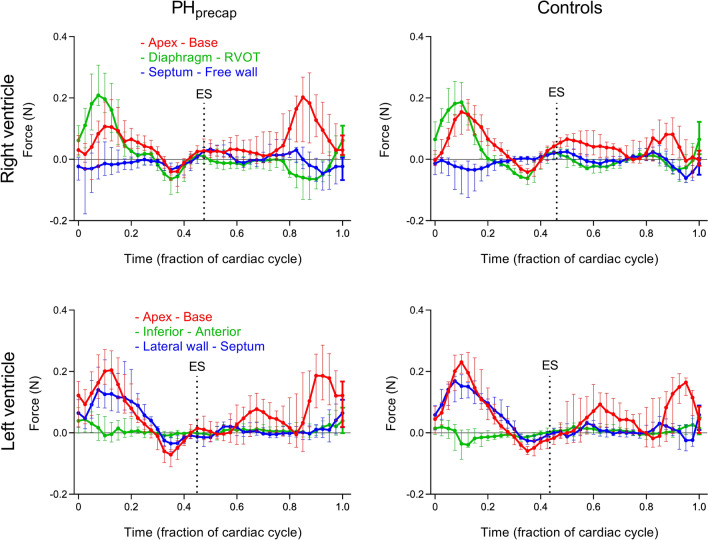
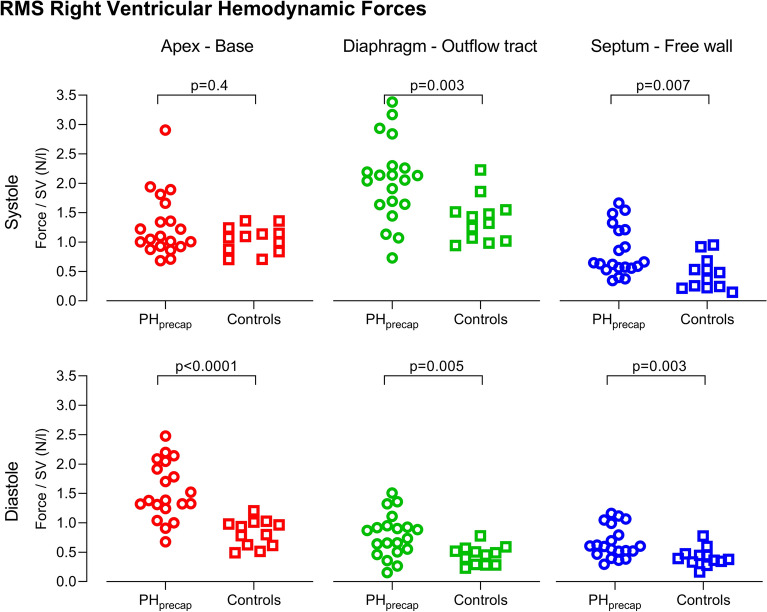
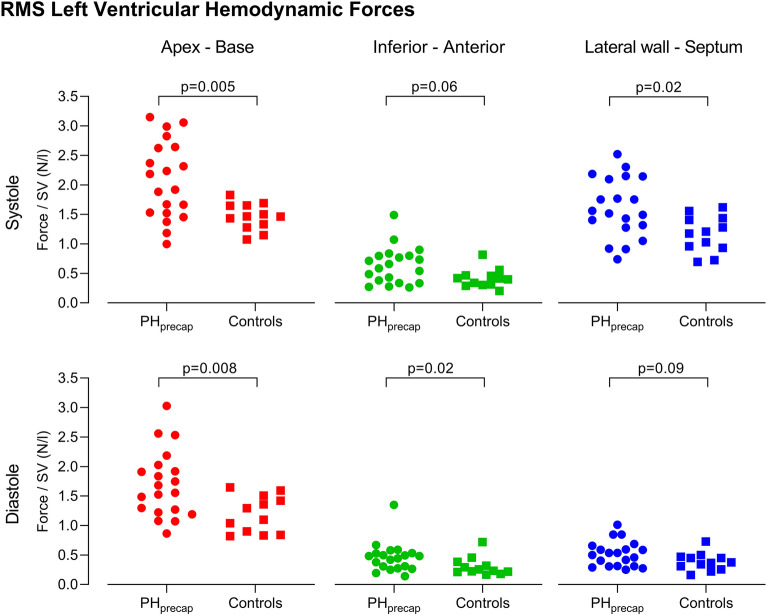
Precapillary pulmonary hypertension (PHprecap) is a condition with elevated pulmonary vascular pressure and resistance. Patients have a poor prognosis and understanding the underlying pathophysiological mechanisms is crucial to guide and improve treatment. Ventricular hemodynamic forces (HDF) are a potential early marker of cardiac dysfunction, which may improve evaluation of treatment effect. Therefore, we aimed to investigate if HDF differ in patients with PHprecap compared to healthy controls. Patients with PHprecap (n = 20) and age- and sex-matched healthy controls (n = 12) underwent cardiac magnetic resonance imaging including 4D flow. Biventricular HDF were computed in three spatial directions throughout the cardiac cycle using the Navier-Stokes equations. Biventricular HDF (N) indexed to stroke volume (l) were larger in patients than controls in all three directions. Data is presented as median N/l for patients vs controls. In the RV, systolic HDF diaphragm-outflow tract were 2.1 vs 1.4 (p = 0.003), and septum-free wall 0.64 vs 0.42 (p = 0.007). Diastolic RV HDF apex-base were 1.4 vs 0.87 (p < 0.0001), diaphragm-outflow tract 0.80 vs 0.47 (p = 0.005), and septum-free wall 0.60 vs 0.38 (p = 0.003). In the LV, systolic HDF apex-base were 2.1 vs 1.5 (p = 0.005), and lateral wall-septum 1.5 vs 1.2 (p = 0.02). Diastolic LV HDF apex-base were 1.6 vs 1.2 (p = 0.008), and inferior-anterior 0.46 vs 0.24 (p = 0.02). Hemodynamic force analysis conveys information of pathological cardiac pumping mechanisms complementary to more established volumetric and functional parameters in precapillary pulmonary hypertension. The right ventricle compensates for the increased afterload in part by augmenting transverse forces, and left ventricular hemodynamic abnormalities are mainly a result of underfilling rather than intrinsic ventricular dysfunction.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
