

Polypharmacy and risk of mortality among patients with heart failure following hospitalization: a nested case-control study
- PMID: 36402903
- PMCID: PMC9675839
- DOI: 10.1038/s41598-022-24285-4
Polypharmacy and risk of mortality among patients with heart failure following hospitalization: a nested case-control study
Abstract
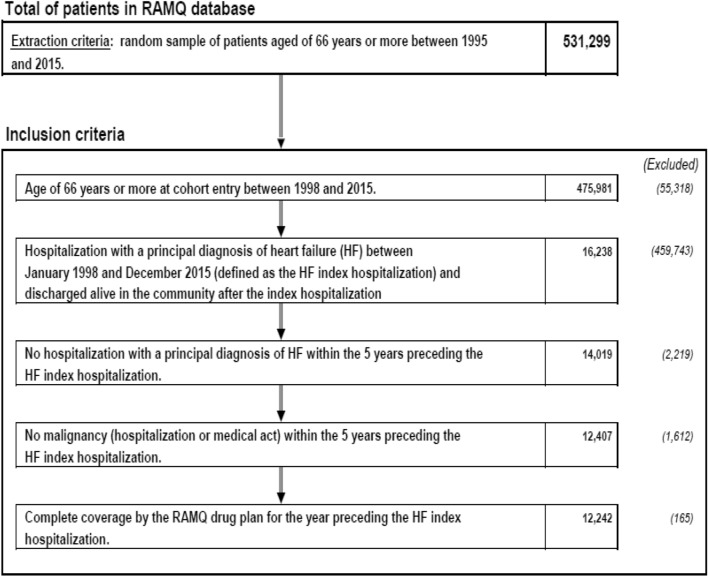
Heart failure (HF) is associated with morbidity, rehospitalization and polypharmacy. The incidence rate of mortality in HF patients with polypharmacy is poorly studied. We examine the association of polypharmacy with mortality risk in incident hospitalized HF patients with a primary diagnosis after discharge from the hospital using Quebec administrative databases, Canada from 1999 to 2015. Polypharmacy, cardiovascular (CV) polypharmacy and non-CV polypharmacy were respectively defined as exposure to ≥ 10 drugs, ≥ 5 CV drugs and ≥ 5 non-CV drugs within three months prior to the case or the control selection date. We conducted a nested case-control study to estimate rate ratios (RR) of all-cause mortality using a multivariate conditional logistic regression during one-year of follow-up. We identified 12,242 HF patients with a mean age of 81.6 years. Neither CV polypharmacy (RR 0.97, 95%CI 0.82-1.15) nor non-CV polypharmacy (RR 0.93, 95%CI 0.77-1.12) were associated with lower mortality risk. However, all polypharmacy (RR 1.31, 95%CI 1.07-1.61) showed an association with mortality risk. Myocardial infarction, valvular disease, peripheral artery disease, diabetes, major bleeding, chronic kidney disease, high comorbidity score, high Frailty score, hydralazine and spironolactone users were associated with increasing mortality risk, ranging from 15 to 61%, while use of angiotensin II inhibitors, beta-blockers, statins, anticoagulant, and antiplatelets were associated with lower risk, ranging from 23 to 32%.
© 2022. The Author(s).
Conflict of interest statement
The authors have no non-financial interests to declare that are relevant to the content of this article. S.P. has received research support from the
Figures
References
-
- Hunt SA, et al. 2009 Focused update incorporated into the ACC/AHA 2005 Guidelines for the diagnosis and management of heart failure in adults: A report of the American College of Cardiology Foundation/American Heart Association task force on practice guidelines developed in collaboration with the International Society for Heart and Lung Transplantation. J. Am. Coll. Cardiol. 2009;53:e1–e90. doi: 10.1016/j.jacc.2008.11.013. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
