

A case report of atypical anti-glomerular basement membrane disease
- PMID: 36402968
- PMCID: PMC9675149
- DOI: 10.1186/s12882-022-03007-y
A case report of atypical anti-glomerular basement membrane disease
Abstract
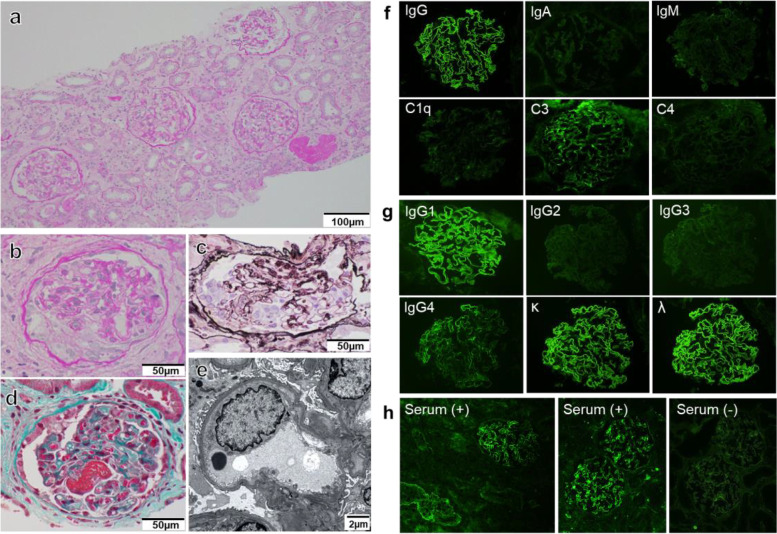
Background: Anti-glomerular basement membrane (anti-GBM) disease is characterized by crescentic necrotizing glomerulonephritis, with linear deposits of immunoglobulin G (IgG) in the GBM. Classic anti-GBM disease is clinically associated with rapidly progressive glomerulonephritis with or without pulmonary hemorrhage. Some patients have a better renal prognosis and milder symptoms than those with classic anti-GBM disease, which is termed atypical anti-GBM disease.
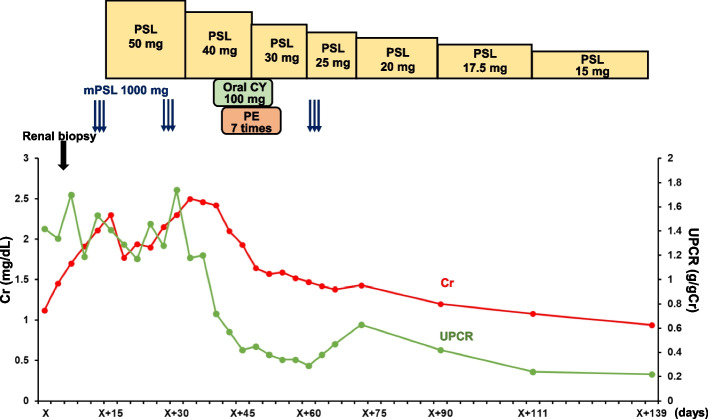
Case presentation: A 43-year-old Japanese woman was admitted to our hospital complaining of hematuria that had persisted for more than one month. Serological examination revealed negativity for anti-nuclear, anti-neutrophilic cytoplasmic, and anti-GBM antibodies. However, renal biopsy showed cellular crescents. Immunofluorescence revealed strong diffuse linear capillary loop staining for IgG. An indirect immunofluorescence antibody method was performed by applying the patient serum to normal kidney tissue to confirm the presence of autoantibodies binding to the GBM. Using this method, anti-GBM antibodies were detected. The patient was treated with high-dose steroids, cyclophosphamide, and plasma exchange. Aggressive treatment resolved proteinuria and hematuria and improved renal function.
Conclusions: Renal biopsy is crucial in the diagnosis of anti-GBM disease, especially when serological tests are negative. Accurately identifying the presence of anti-GBM disease is important to initiate optimal treatment.
Keywords: Atypical anti-GBM disease; Indirect immunofluorescence antibody method; Linear deposits of IgG.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
A case of aggressive atypical anti-GBM disease complicated by CMV pneumonitis.BMC Nephrol. 2019 Jan 31;20(1):29. doi: 10.1186/s12882-019-1227-z. BMC Nephrol. 2019. PMID: 30704432 Free PMC article.
-
Development of anti-glomerular basement membrane glomerulonephritis during the course of IgA nephropathy: a case report.BMC Nephrol. 2019 Jan 25;20(1):25. doi: 10.1186/s12882-019-1207-3. BMC Nephrol. 2019. PMID: 30683055 Free PMC article.
-
Atypical Anti-Glomerular Basement Membrane Nephritis: A Case Series From the French Nephropathology Group.Am J Kidney Dis. 2024 Jun;83(6):713-728.e1. doi: 10.1053/j.ajkd.2023.11.003. Epub 2024 Jan 1. Am J Kidney Dis. 2024. PMID: 38171412
-
High-frequency plasma exchange therapy for immunocompromised, type I crescentic glomerulonephritis complicated with IgA nephropathy: A case report and literature review.Medicine (Baltimore). 2023 Jan 20;102(3):e32698. doi: 10.1097/MD.0000000000032698. Medicine (Baltimore). 2023. PMID: 36701698 Free PMC article. Review.
-
A rare case of sero-negative anti-glomerular basement membrane disease combined with diabetic nephropathy and literature review.Ren Fail. 2025 Dec;47(1):2537808. doi: 10.1080/0886022X.2025.2537808. Epub 2025 Aug 10. Ren Fail. 2025. PMID: 40785208 Free PMC article. Review.
Cited by
-
Anti-GBM disease with positive serum anti-GBM antibodies but negative IgG deposition: A case report.SAGE Open Med Case Rep. 2023 Jul 31;11:2050313X231189767. doi: 10.1177/2050313X231189767. eCollection 2023. SAGE Open Med Case Rep. 2023. PMID: 37533486 Free PMC article.
-
Atypical Anti-Glomerular Basement Membrane Disease.Kidney Int Rep. 2023 Mar 21;8(6):1151-1161. doi: 10.1016/j.ekir.2023.03.010. eCollection 2023 Jun. Kidney Int Rep. 2023. PMID: 37284681 Free PMC article. Review.
-
Anti-GBM Nephritis in an 11-Year-Old Female Child: A Rare Case Report.Cureus. 2024 Aug 25;16(8):e67736. doi: 10.7759/cureus.67736. eCollection 2024 Aug. Cureus. 2024. PMID: 39318945 Free PMC article.
-
Atypical anti-glomerular basement membrane disease with membranous hyperplasia: diagnostic challenges and treatment variability.BMC Nephrol. 2024 Apr 15;25(1):132. doi: 10.1186/s12882-024-03571-5. BMC Nephrol. 2024. PMID: 38622525 Free PMC article.
-
Atypical Anti-glomerular Basement Membrane Disease in a 16-Year-Old Male Child: A Case Report.Cureus. 2025 Feb 6;17(2):e78644. doi: 10.7759/cureus.78644. eCollection 2025 Feb. Cureus. 2025. PMID: 40062063 Free PMC article.
References
-
- Koyama A, Yamagata K, Makino H, Arimura Y, Wada T, Nitta K, Nihei H, Muso E, Taguma Y, Shigematsu H, Sakai H, Japan RPGN Registry Group A nationwide survey of rapidly progressive glomerulonephritis in Japan: etiology, prognosis and treatment diversity. Clin Exp Nephrol. 2009;13(6):633–650. doi: 10.1007/s10157-009-0201-7. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
