

Carotid artery corrected flow time and respiratory variations of peak blood flow velocity for prediction of hypotension after induction of general anesthesia in elderly patients
- PMID: 36402973
- PMCID: PMC9675965
- DOI: 10.1186/s12877-022-03619-x
Carotid artery corrected flow time and respiratory variations of peak blood flow velocity for prediction of hypotension after induction of general anesthesia in elderly patients
Abstract
Background: Postinduction hypotension is closely related to postoperative complications. Elderly patients with compromised cardiovascular compensatory reserve are more susceptible to hypotension after induction of general anesthesia. This study investigated whether the carotid artery corrected flow time (FTc) and respiratory variation of peak blood flow velocity in the common carotid artery (ΔVpeak) could predict postinduction hypotension in elderly patients.
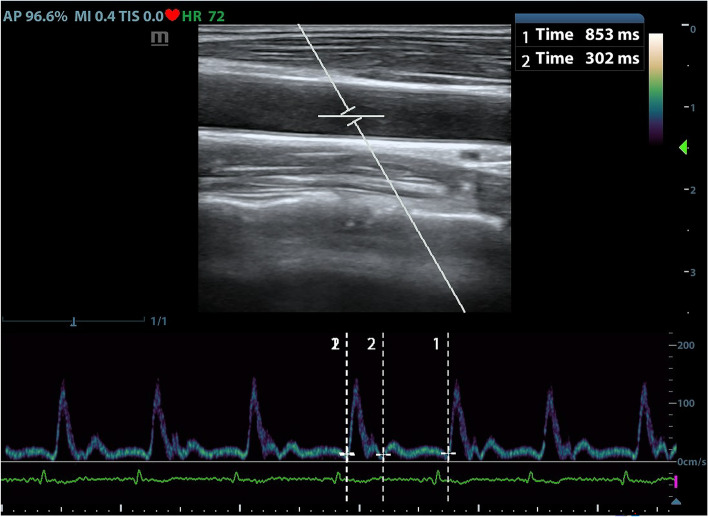
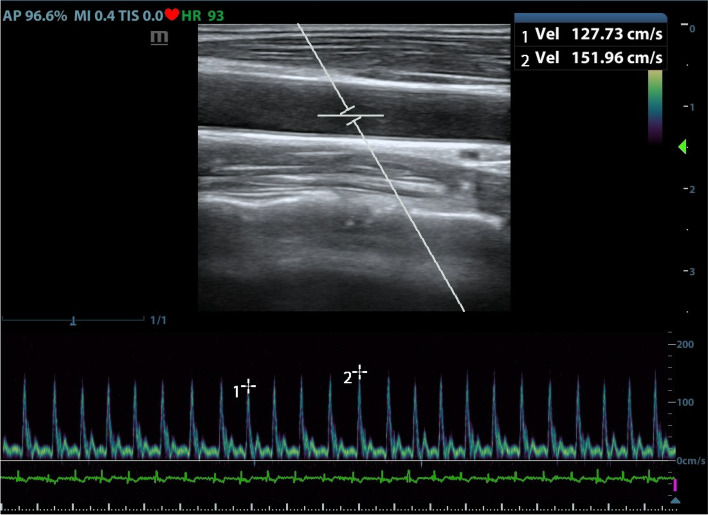
Methods: This prospective observational study included elderly patients aged 65 to 75 who were scheduled for elective surgery under general anesthesia with ASA physical status class of I-II, without cardiovascular disease, hypertension, diabetes, or obesity. Anesthesia was induced by midazolam, sufentanil, and etomidate and was maintained by sevoflurane. The carotid artery FTc and ΔVpeak were measured by ultrasound before induction of anesthesia. Hemodynamic data were recorded before induction and then during the first 10 min after induction.
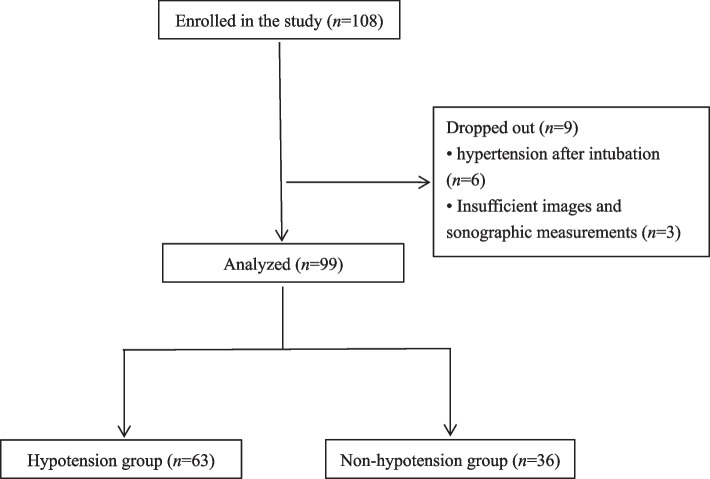
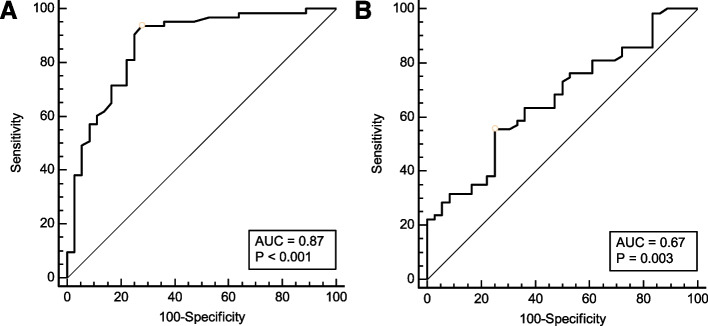
Results: Ninety-nine patients were included in the final analysis, of whom 63 developed postinduction hypotension. The area under the receiver operating characteristic curves was 0.87 (0.78 to 0.93) for carotid artery FTc and 0.67 (0.56 to 0.76) for ΔVpeak, respectively. The optimal cutoff value for predicting postinduction hypotension was 379.1 ms for carotid artery FTc, with sensitivity and specificity of 72.2 and 93.7%, respectively. The best cutoff value was 7.5% for ΔVpeak, with sensitivity and specificity of 55.6 and 75.0%, respectively.
Conclusions: The carotid artery FTc is a reliable predictor of postinduction hypotension in elderly patients with ASA status of I or II, without cardiovascular disease, hypertension, diabetes, or obesity. Elderly patients with a carotid artery FTc less than 379.1 ms before anesthesia have a higher risk of postinduction hypotension.
Trial registration: Clinical Trial Registry on August 2nd, 2020 ( www.chictr.org.cn ; ChiCTR2000035190).
Keywords: Blood flow velocity; Carotid Doppler ultrasound; Corrected flow time; Elderly; General anesthesia; Postinduction hypotension; Respiration.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Salmasi V, Maheshwari K, Yang D, et al. Relationship between intraoperative hypotension, defined by either reduction from baseline or absolute thresholds, and acute kidney and myocardial injury after noncardiac surgery: a retrospective cohort analysis. Anesthesiology. 2017;126(1):47–65. doi: 10.1097/ALN.0000000000001432. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
