

Present and future directions in diabetic kidney disease
- PMID: 36403478
- PMCID: PMC9764992
- DOI: 10.1016/j.jdiacomp.2022.108357
Present and future directions in diabetic kidney disease
Abstract
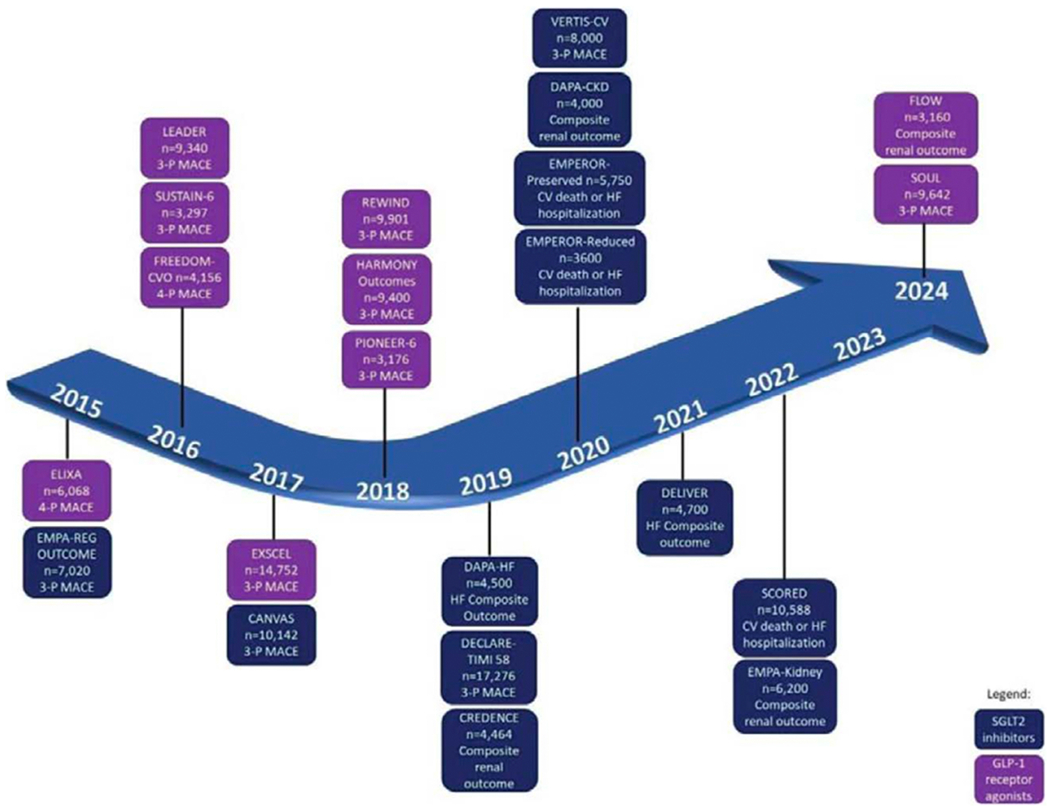
Diabetic kidney disease (DKD) is the leading cause of kidney failure and is associated with substantial risk of cardiovascular disease, morbidity, and mortality. Traditionally, DKD prevention and management have focused on addressing hyperglycemia, hypertension, obesity, and renin-angiotensin system activation as important risk factors for disease. Over the last decade, sodium-glucose cotransporter-2 inhibitors and glucagon-like peptide-1 receptor agonists have been shown to meaningfully reduce risk of diabetes-related kidney and cardiovascular complications. Additional agents demonstrating benefit in DKD such as non-steroidal mineralocorticoid receptor antagonists and endothelin A receptor antagonists are further contributing to the growing arsenal of DKD therapies. With the availability of greater therapeutic options comes the opportunity to individually optimize DKD prevention and management. Novel applications of transcriptomic, proteomic, and metabolomic/lipidomic technologies, as well as use of artificial intelligence and reinforced learning methods through consortia such as the Kidney Precision Medicine Project and focused studies in established cohorts hold tremendous promise for advancing our understanding and treatment of DKD. Specifically, enhanced understanding of the molecular mechanisms underlying DKD pathophysiology may allow for the identification of new mechanism-based DKD subtypes and the development and implementation of targeted therapies. Implementation of personalized care approaches has the potential to revolutionize DKD care.
Keywords: Chronic kidney disease; Diabetic kidney disease; Omics; Precision medicine.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest CPL has nothing to disclose. M.K. reports grants from NIH/NIDDK and JDRF in support of this manuscript. Grants and contracts outside the submitted work through the University of Michigan with NIH, Chan Zuckerberg Initiative, AstraZeneca, NovoNordisk, Eli Lilly, Gilead, Goldfinch Bio, Janssen, Boehringer-Ingelheim, Moderna, European Union Innovative Medicine Initiative, Certa, Chinook, amfAR, Angion, RenalytixAI, Travere, Regeneron, IONIS, consulting fees through the University of Michigan from Astellas, Poxel, Janssen and UCB. In addition, M.K. has a patent PCT/EP2014/073413 “Biomarkers and methods for progression prediction for chronic kidney disease” licensed. SP has nothing to disclose. RPB consults for Novo Nordisk and Roche. IHdB consults for AstraZeneca, Bayer, Boehringer-Ingelheim, Cyclerion Therapeutics, George Clinical, Goldfinch Bio, Ironwood, Lilly, Otsuka and receives research equipment and supplies from DexCom.
Figures

References
-
- International Diabetes Federation. IDF Diabetes Atlas, 10th Edn. Vol 102. (International Diabetes Federation, ed.).; 2021. doi:10.1016/j.diabres.2013.10.013 - DOI
Publication types
MeSH terms
Substances
Grants and funding
- U24 DK076169/DK/NIDDK NIH HHS/United States
- U24 DK115255/DK/NIDDK NIH HHS/United States
- U2C DK114886/DK/NIDDK NIH HHS/United States
- U01 DK133090/DK/NIDDK NIH HHS/United States
- R24 DK082841/DK/NIDDK NIH HHS/United States
- P30 DK089503/DK/NIDDK NIH HHS/United States
- R01 DK132399/DK/NIDDK NIH HHS/United States
- U01 DK133081/DK/NIDDK NIH HHS/United States
- R01 DK126373/DK/NIDDK NIH HHS/United States
- P30 DK020572/DK/NIDDK NIH HHS/United States
- P30 DK081943/DK/NIDDK NIH HHS/United States
- R01 DK125084/DK/NIDDK NIH HHS/United States
- U24 DK114886/DK/NIDDK NIH HHS/United States
- R01 DK116723/DK/NIDDK NIH HHS/United States
- U01 DK119083/DK/NIDDK NIH HHS/United States
- P30 DK035816/DK/NIDDK NIH HHS/United States
- R01 DK107956/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
