

Neuroimaging Patterns of Intracranial Infections: Meningitis, Cerebritis, and Their Complications
- PMID: 36404039
- PMCID: PMC10904173
- DOI: 10.1016/j.nic.2022.07.001
Neuroimaging Patterns of Intracranial Infections: Meningitis, Cerebritis, and Their Complications
Abstract
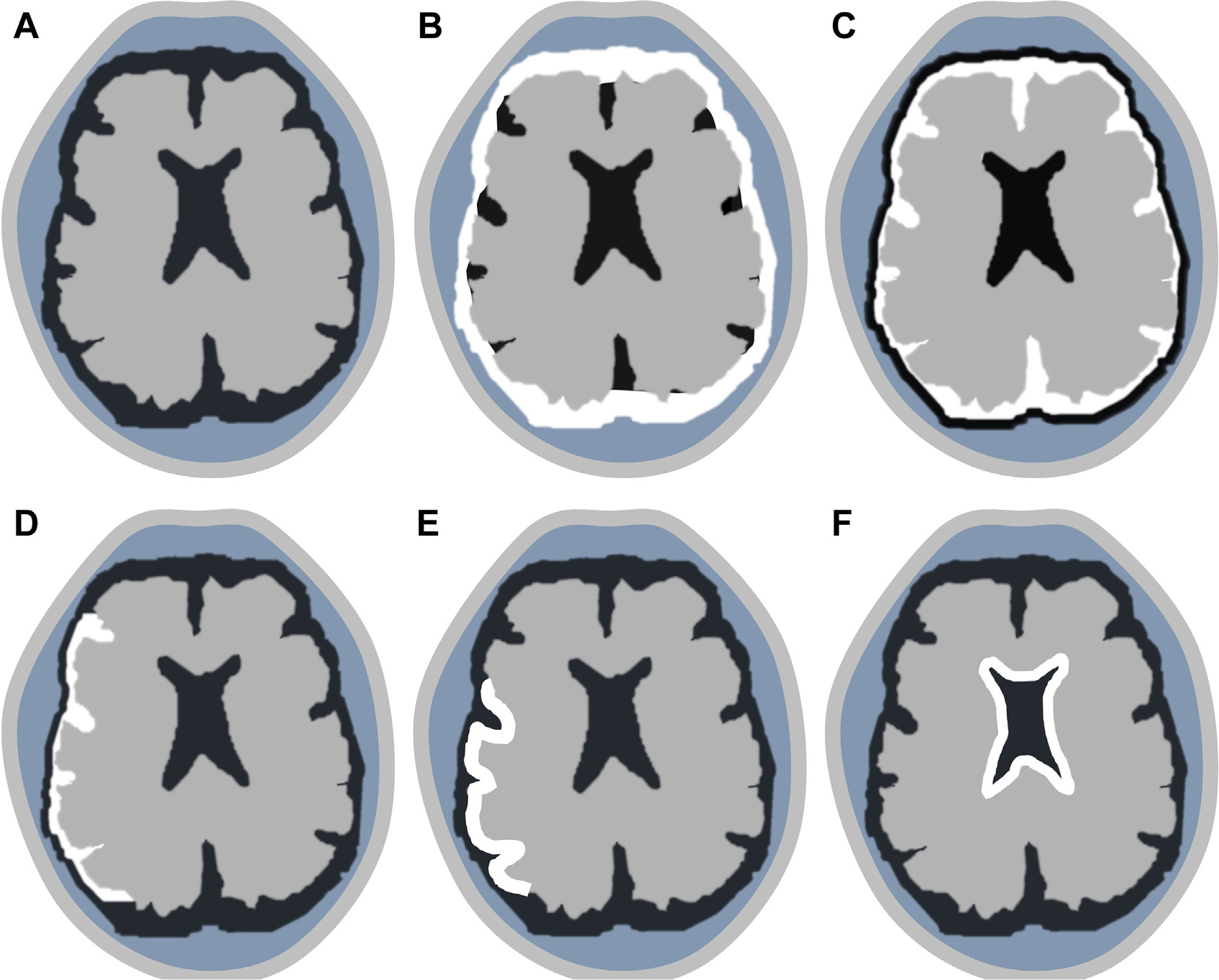
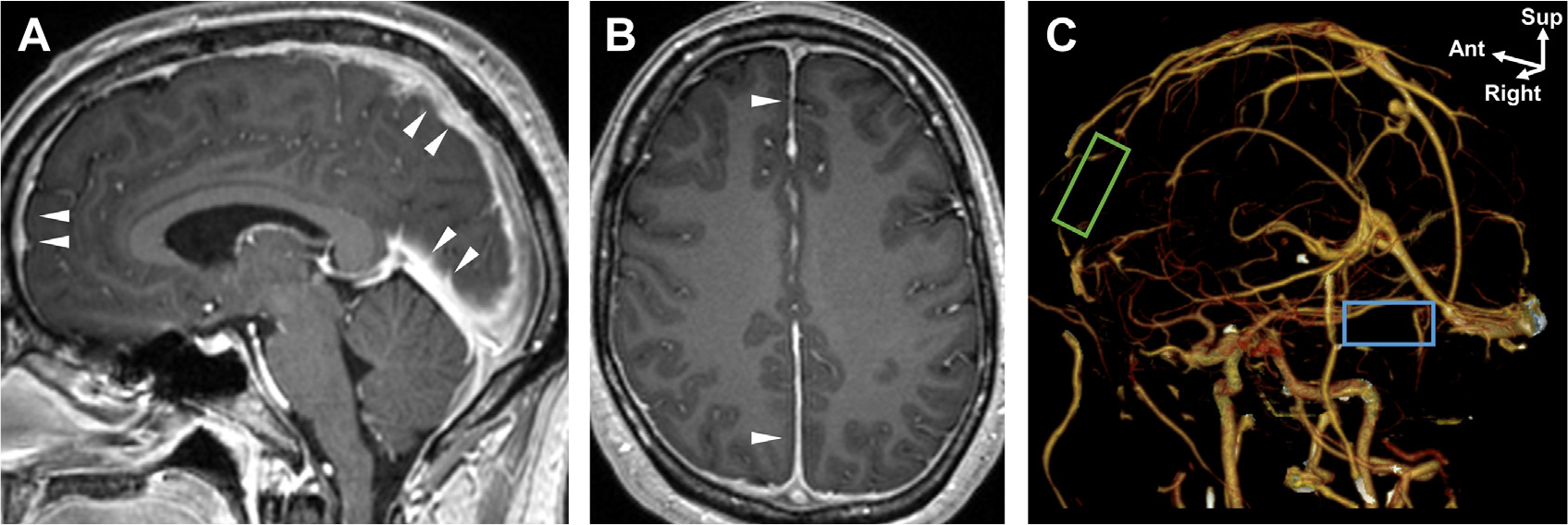
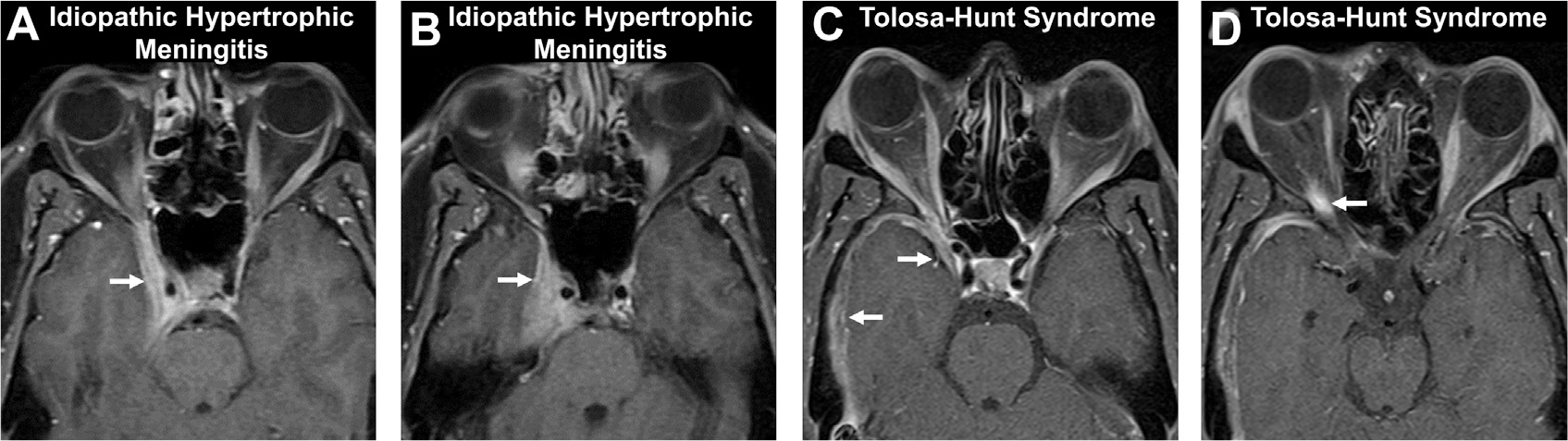
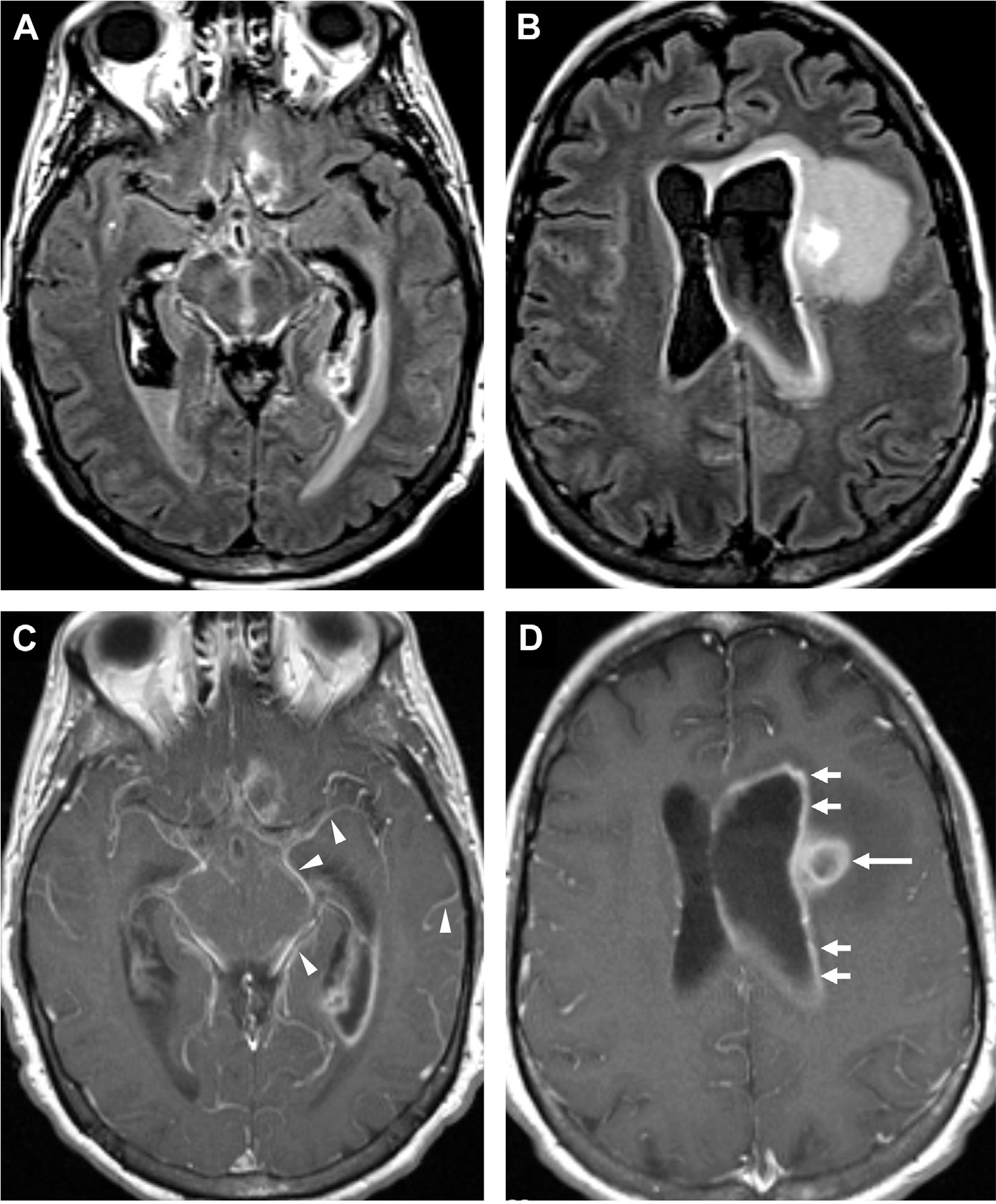
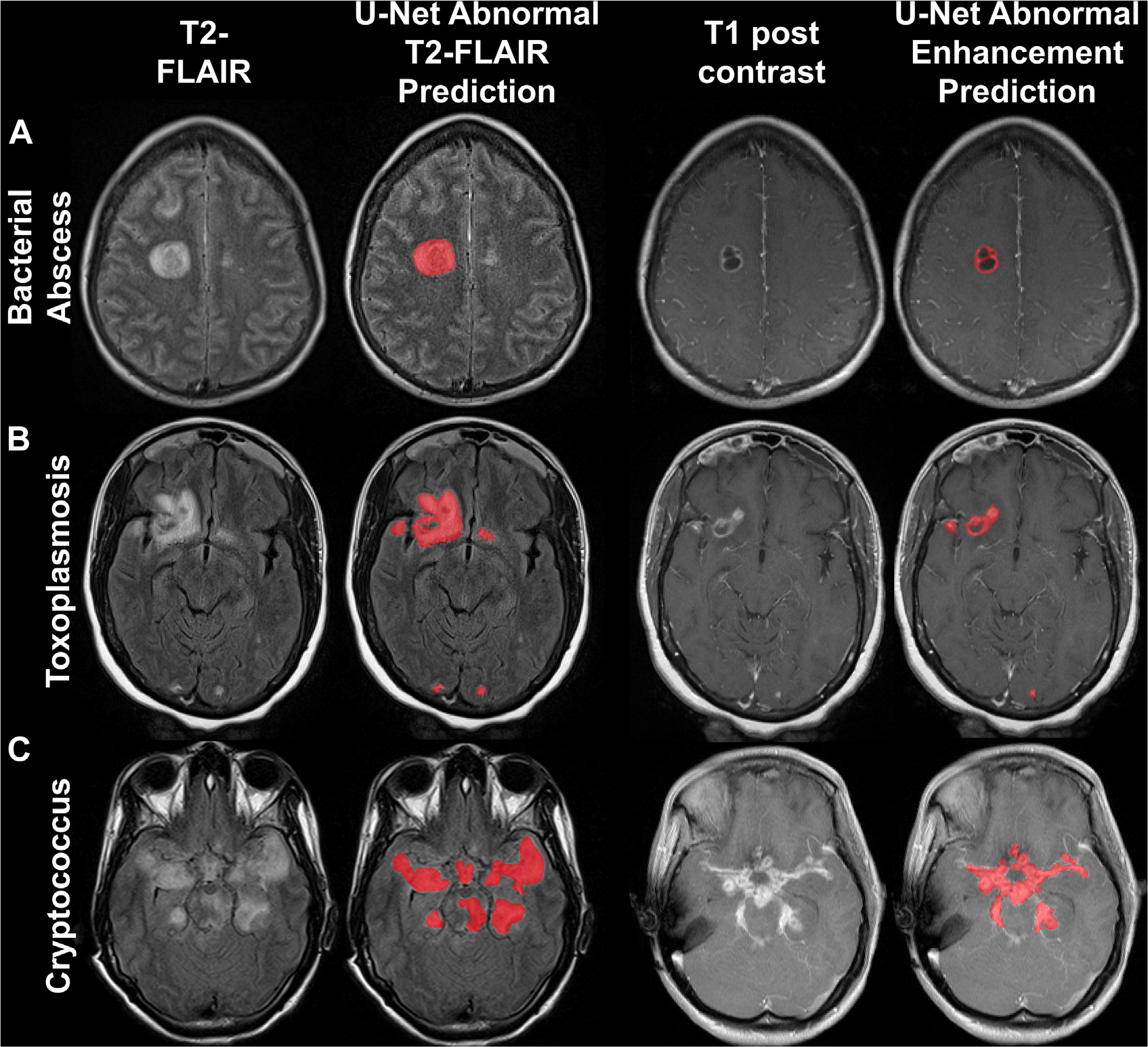
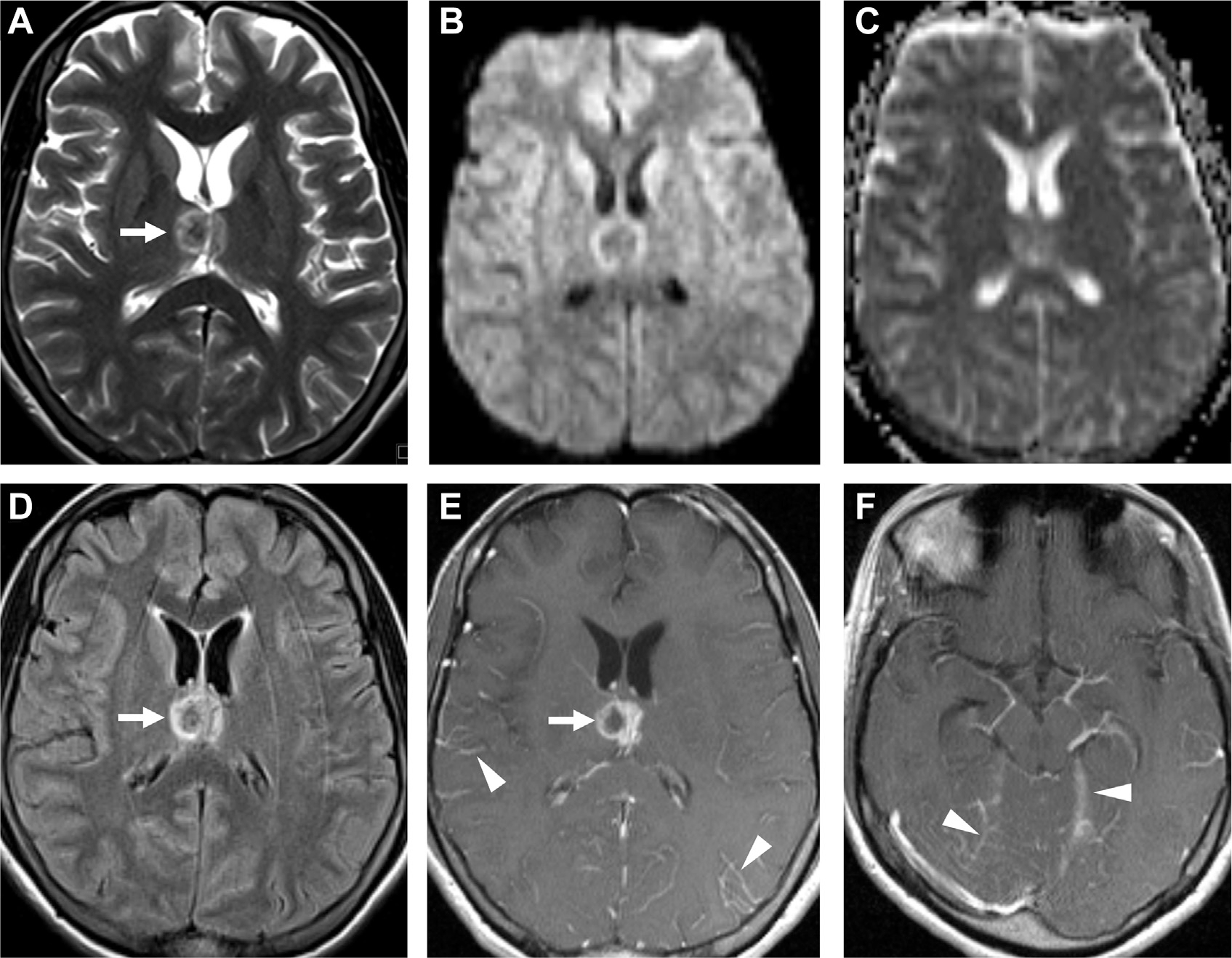
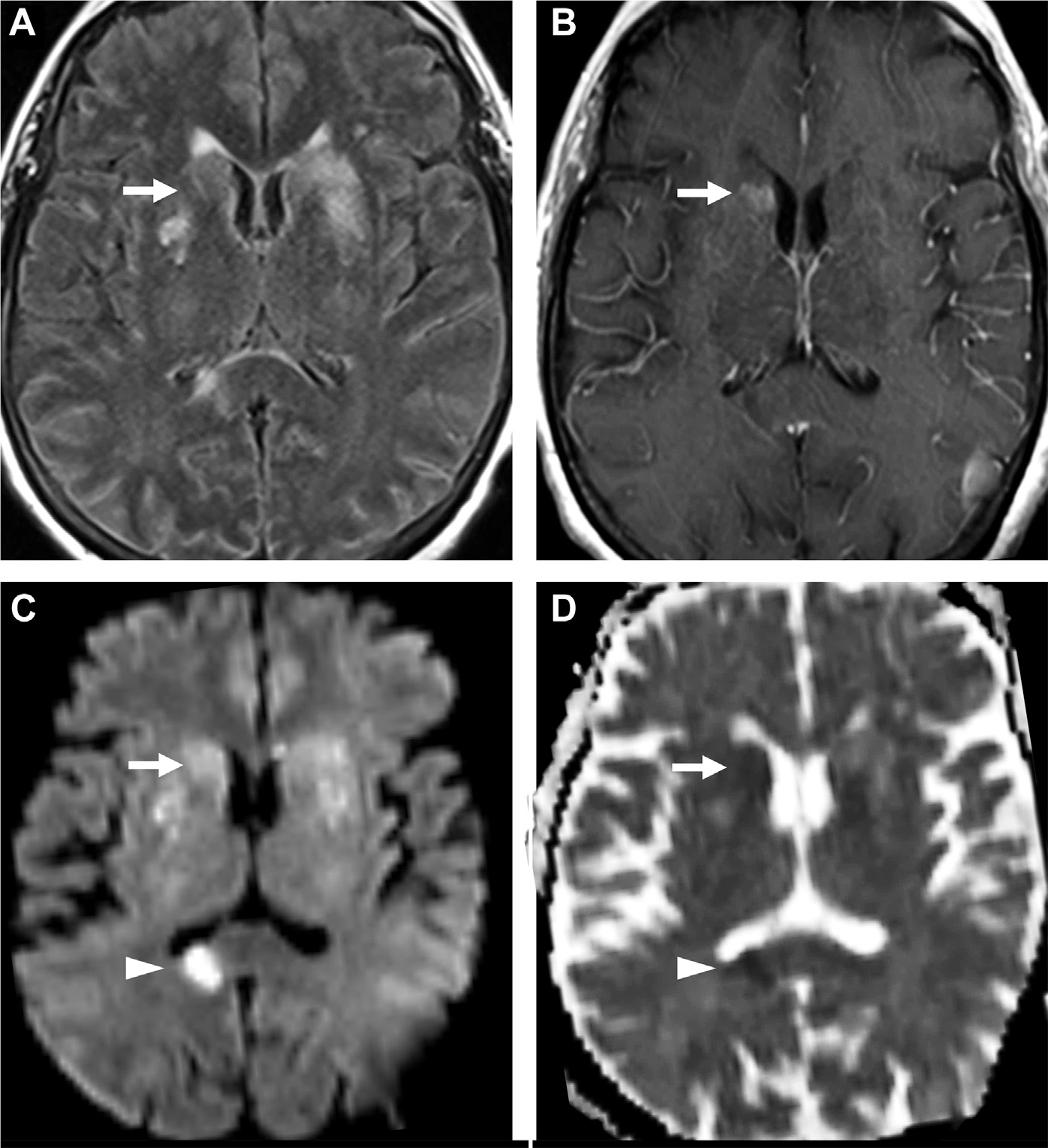
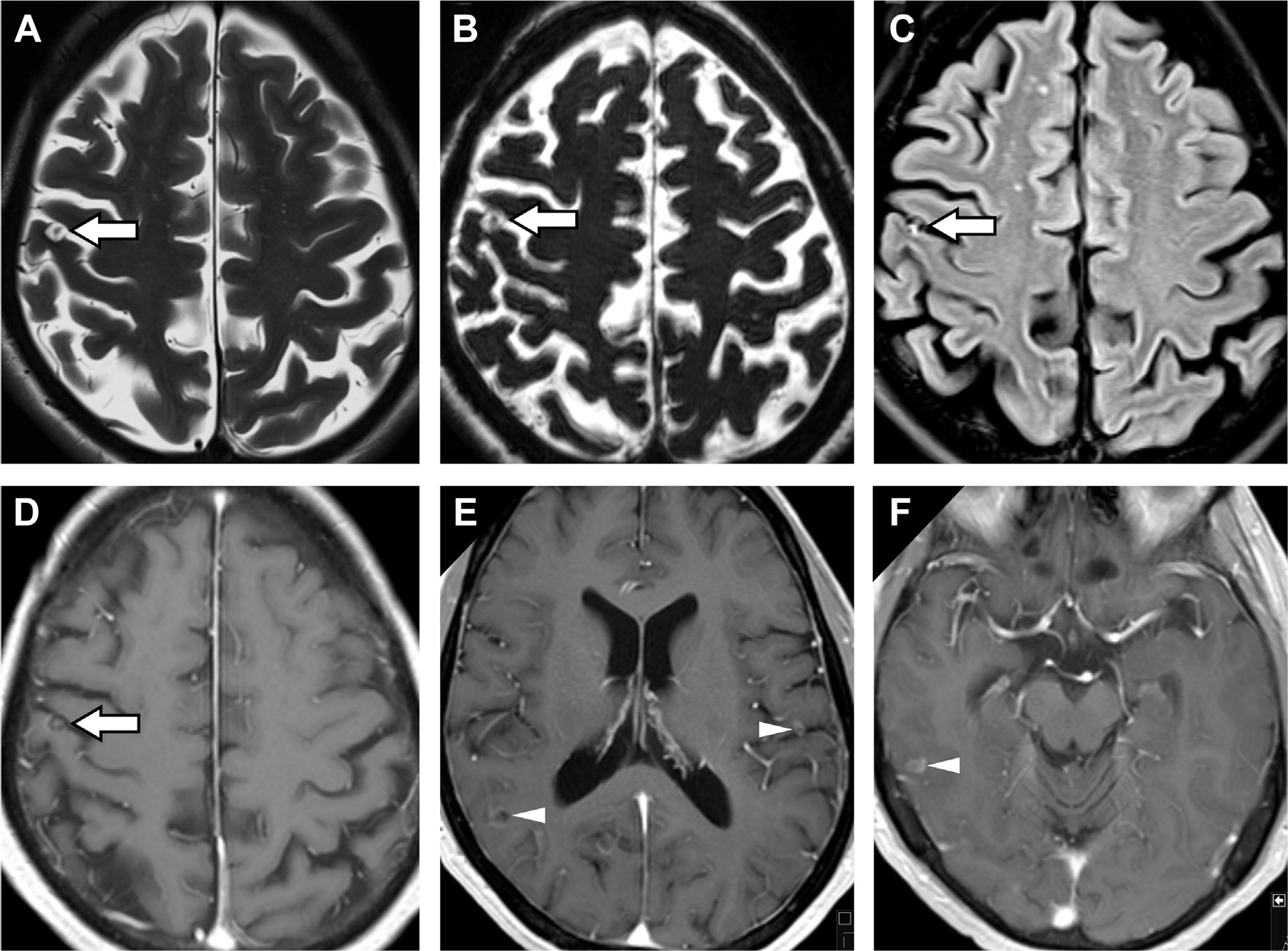
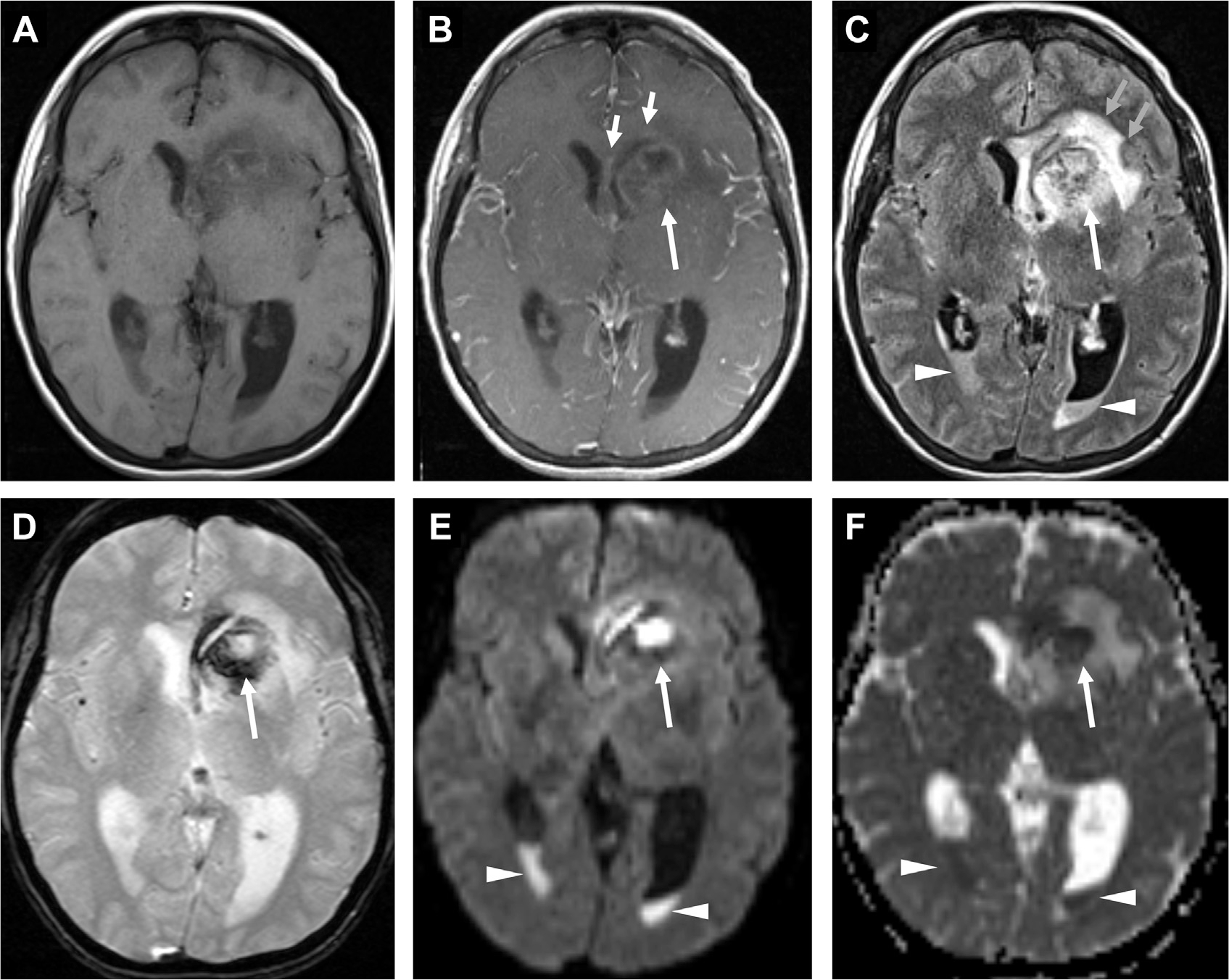
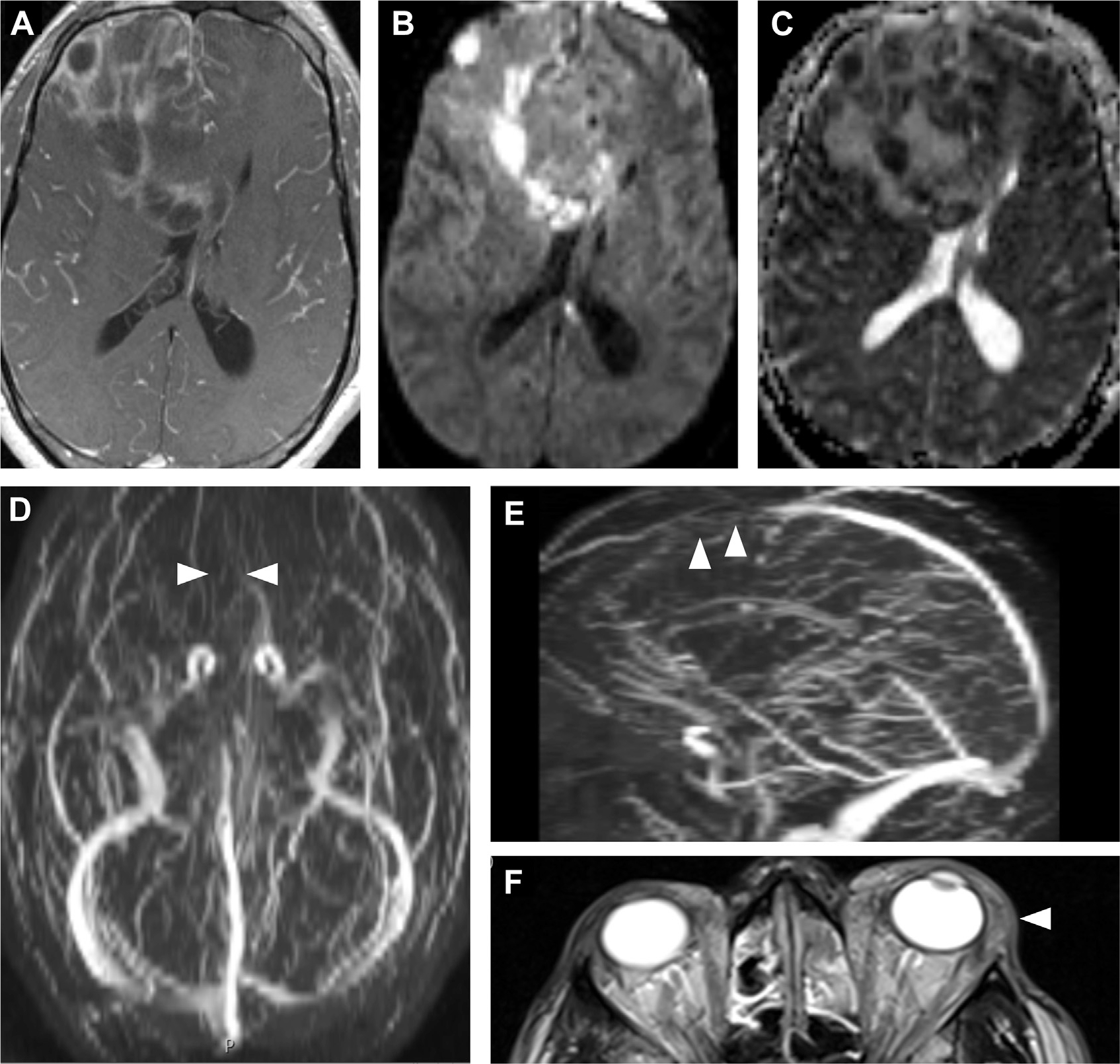
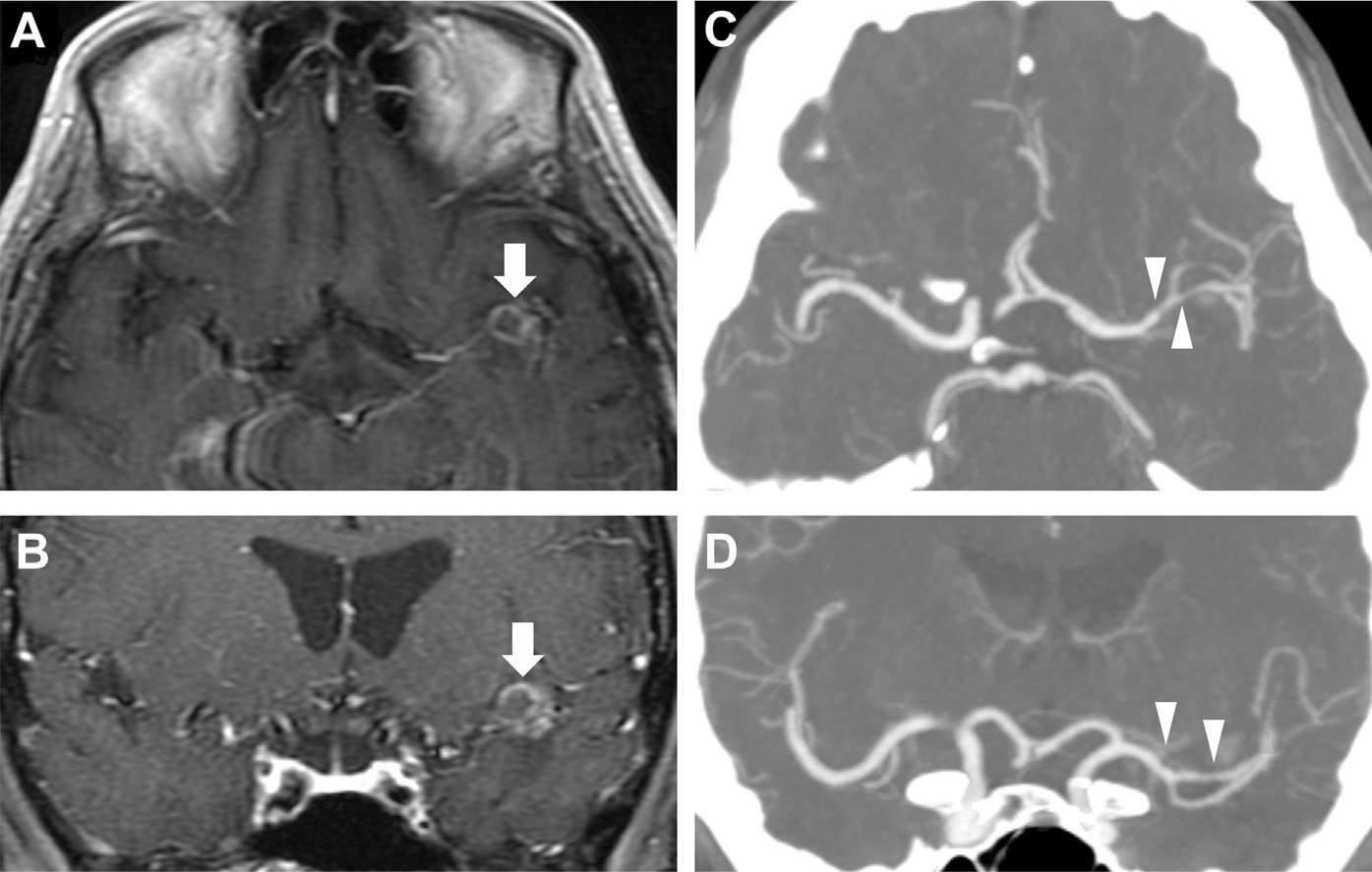
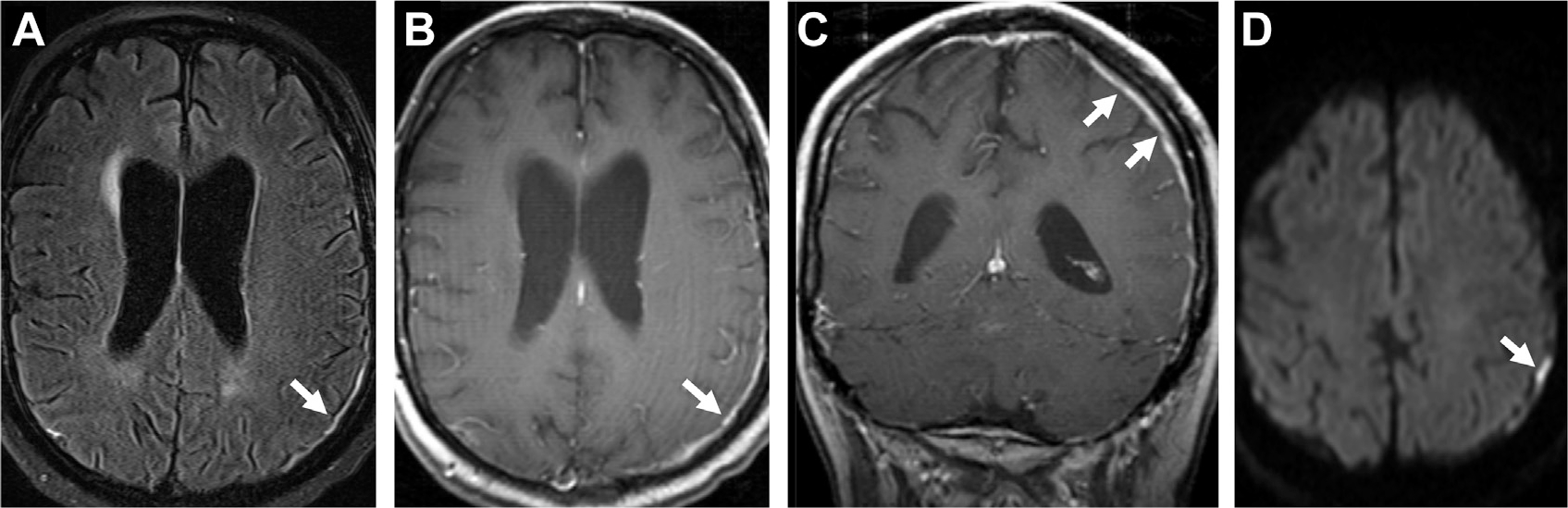
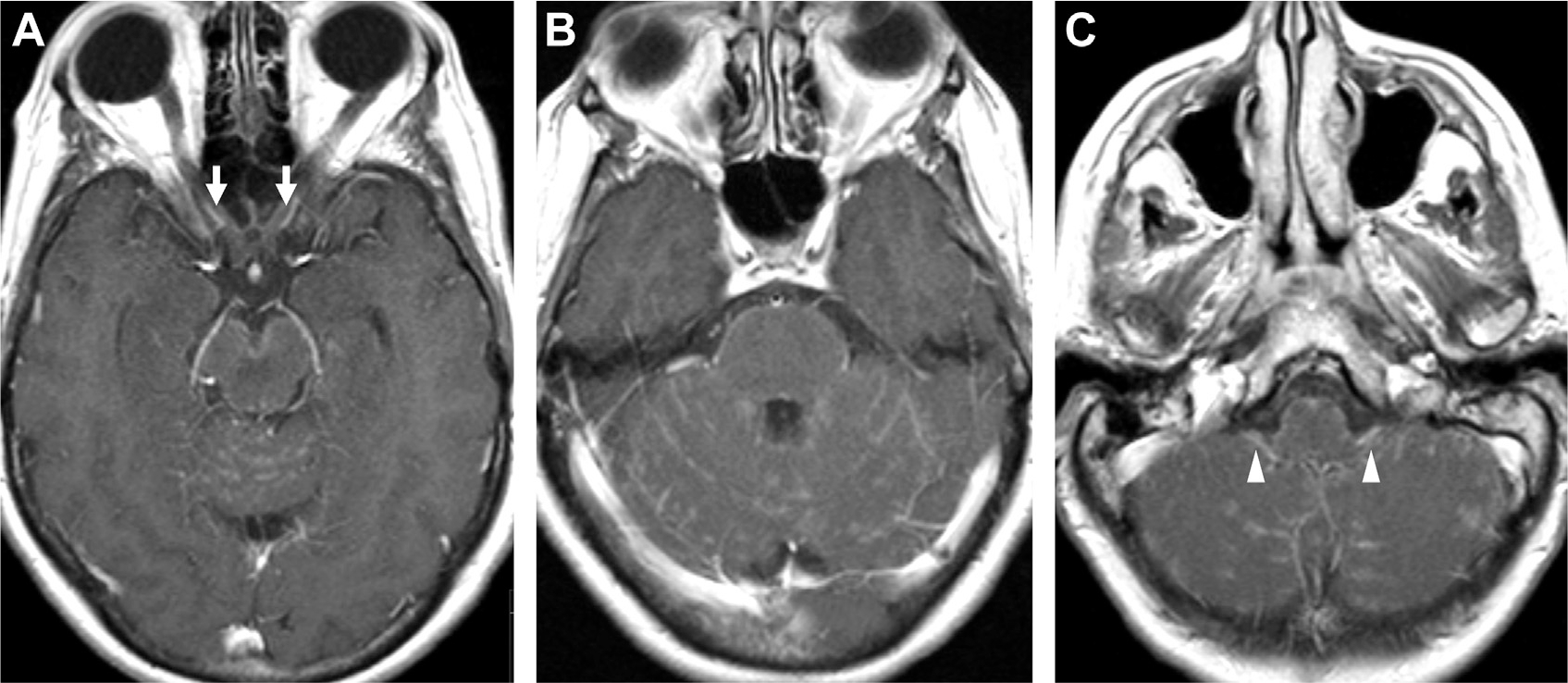
Neuroimaging provides rapid, noninvasive visualization of central nervous system infections for optimal diagnosis and management. Generalizable and characteristic imaging patterns help radiologists distinguish different types of intracranial infections including meningitis and cerebritis from a variety of bacterial, viral, fungal, and/or parasitic causes. Here, we describe key radiologic patterns of meningeal enhancement and diffusion restriction through profiles of meningitis, cerebritis, abscess, and ventriculitis. We discuss various imaging modalities and recent diagnostic advances such as deep learning through a survey of intracranial pathogens and their radiographic findings. Moreover, we explore critical complications and differential diagnoses of intracranial infections.
Keywords: Abscess; Central nervous system; Cerebritis; Glymphatics; Infection; Meningitis; Neuroimaging; Ventriculitis.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure S. Mohan has grant funding from the National Cancer Institute (NCI R01 CA262584), Galileo CDS and Novocure, USA. M. T. Duong has research funding from the National Institute on Aging (NIA F30 AG074524). J. D. Rudie has research support from the National Institute of Biomedical Imaging and Bioengineering (NIBIB T32 EB004311) and Radiological Society of North America (RSNA RR1778) research grant. There are no additional disclosures to report.
Figures
References
-
- Mohan S, Jain KK, Arabi M, et al. Imaging of Meningitis and Ventriculitis. Neuroimaging Clin N Am 2012;22(4):557–83. - PubMed
-
- Rath TJ, Hughes M, Arabi M, et al. Imaging of Cerebritis, Encephalitis, and Brain Abscess. Neuroimaging Clin N Am 2012;22(4):585–607. - PubMed
-
- Mortazavi MM, Tubbs RS, Riech S, et al. Anatomy and pathology of the cranial emissary veins: a review with surgical implications. Neurosurgery 2012;70(5):1312–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
