

AbsorbaTack™ vs. ProTack™ vs. sutures: a biomechanical analysis of cervical fixation methods for laparoscopic apical fixations in the porcine model
- PMID: 36404354
- PMCID: PMC9984508
- DOI: 10.1007/s00404-022-06827-3
AbsorbaTack™ vs. ProTack™ vs. sutures: a biomechanical analysis of cervical fixation methods for laparoscopic apical fixations in the porcine model
Abstract
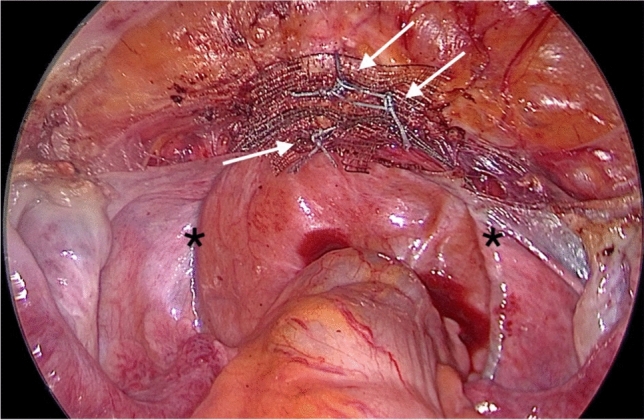
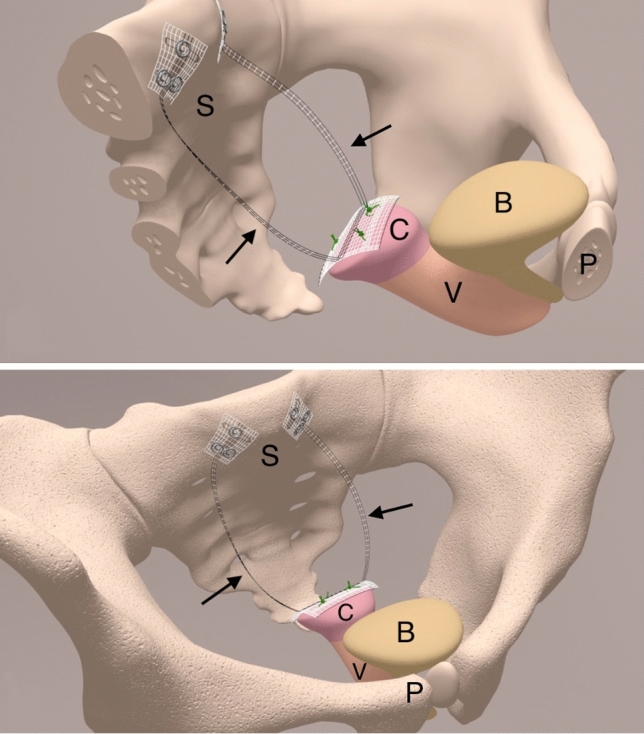
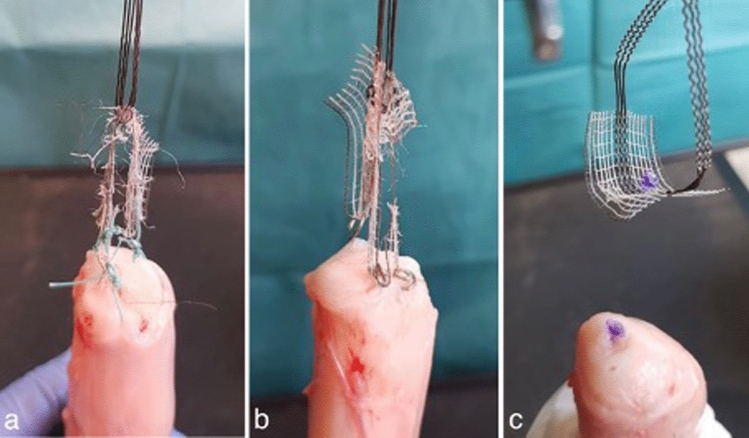
Purpose: Treatment of pelvic organ prolapse (POP) often requires the use of synthetic mesh. In case of a novel and standardized bilateral apical fixation, both uterosacral ligaments are replaced by polyvinylidene-fluoride (PVDF) tapes. One of the main problems remains the fixation method, which should be stable, but also simple and quick to use. The current study evaluated biomechanical differences between the cervical tape fixation with sutures (group 1), non-absorbable tacks (group 2) and absorbable tacks (group 3) in an in vitro porcine model.
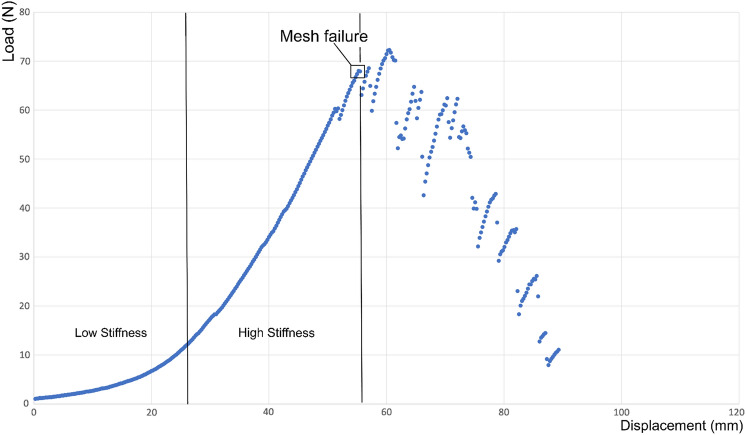
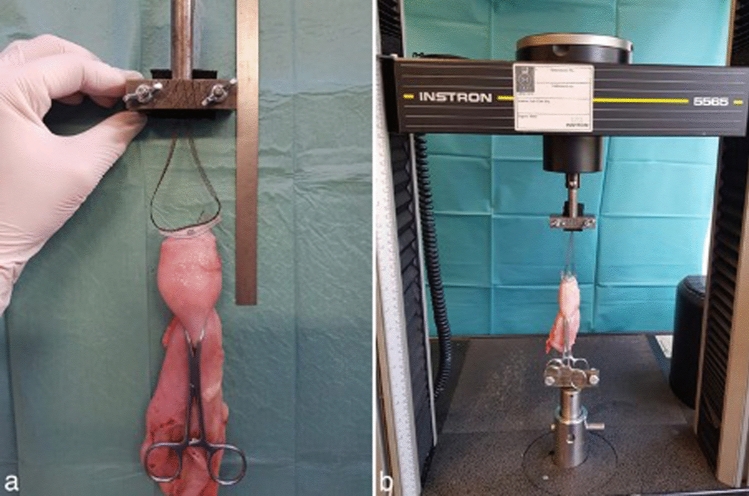
Methods: A total of 28 trials, conducted in three groups, were performed on porcine, fresh cadaver uteri. All trials were performed until mesh, tissue or fixation device failure occurred. Primary endpoints were the biomechanical properties maximum load (N), displacement at failure (mm) and stiffness (N/mm). The failure mode was a secondary endpoint.
Results: There was a significant difference between all three groups concerning the maximum load. Group 1 (sutures) supported a maximum load of 64 ± 15 N, group 2 (non-absorbable tacks) yielded 41 ± 10 N and group 3 (absorbable tacks) achieved 15 ± 8 N. The most common failure mode was a mesh failure for group 1 and 2 and a fixation device failure for group 3.
Conclusion: The PVDF-tape fixation with sutures supports 1.5 times the load that is supported by non-absorbable tacks and 4.2 times the load that is supported by absorbable tacks. Nevertheless, there was also a stable fixation through tacks. Sutures are the significantly stronger and cheaper fixation device but may prolong the surgical time in contrast to the use of tacks.
Keywords: Apical fixation; Biomechanical analysis; Cervicosacropexy; Mesh fixation; Pelvic organ prolapse; Polyvinylidene-fluoride; Uterosacral ligaments.
© 2022. The Author(s).
Conflict of interest statement
Financial interests: for the implementation of the study 40 PVDF-CESA-replacement structures were sponsored by the FEG Textiltechnik mbH Company. Non-financial interests: the authors declare that they have no conflict of interest.
Figures

References
-
- Iglesia CB, Smithling KR. Pelvic Organ Prolapse. Am Fam Physician. 2017;96(3):179–185. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
