

Long-Term Effect of Pancreaticoduodenectomy Combined with Revascularization for Resectable Pancreatic Carcinoma in Elderly Patients
- PMID: 36404606
- PMCID: PMC9695170
- DOI: 10.12659/MSM.938443
Long-Term Effect of Pancreaticoduodenectomy Combined with Revascularization for Resectable Pancreatic Carcinoma in Elderly Patients
Abstract
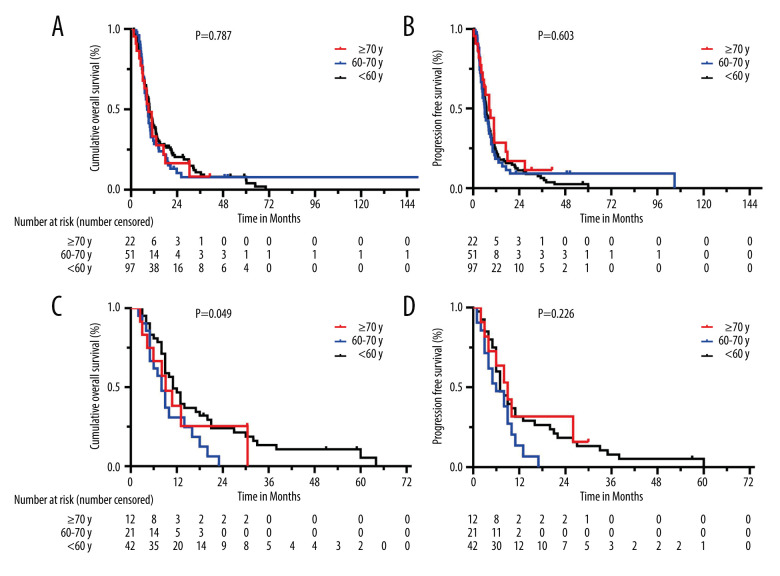
BACKGROUND Pancreaticoduodenectomy combined with revascularization (PDR) is the main surgical procedure for resectable pancreatic ductal adenocarcinoma (PDAC) with venous system invasion, but this procedure is discouraged in elderly patients because of physical complexity. Our aim was to explore the differences of perioperative and survival in patients of different ages who underwent PDR. MATERIAL AND METHODS We reviewed data from PDAC patients undergoing PDR from 2007 to 2018. Patients were subdivided into 3 groups according to age: <60 years, 60-70 years, and ≥70 years. Postoperative complications and long-term survival were compared among the 3 groups. RESULTS From 626 patients, 185 had en bloc venous resection who underwent PDR (103, 55, and 27 patients from young to elderly). Increasing age was linked to a higher prevalence of ICU management (P=0.035) and more serious complications (grade ≥III, P=0.043); overall mortality was 8.1% and did not significantly differ among age-matched groups. Further, there was no difference in overall survival (OS) or progression-free survival (PFS) based on age (<60, 60-70, ≥70, median OS were 9.7, 8.4 vs 9.1 months, respectively, P=0.787; median PFS were 6.9, 6.1 vs 8.4 months, respectively, P=0.603). However, patients <60 years whose tumors invaded the superior mesenteric vascular had better survival outcomes when compared with the other 2 groups (11.5 vs 8.4, 9.1 months, P=0.049). CONCLUSIONS The results show that age should not be considered an absolute contraindication for PDR, as elderly patients can achieve the same surgical efficacy and long-term survival prognosis.
Conflict of interest statement
Figures
Similar articles
-
Long-term outcomes following en bloc resection for pancreatic ductal adenocarcinoma of the head with portomesenteric venous invasion.Asian J Surg. 2021 Jan;44(1):313-320. doi: 10.1016/j.asjsur.2020.07.021. Epub 2020 Sep 21. Asian J Surg. 2021. PMID: 32972828
-
The impact of extent of pancreatic and venous resection on survival for patients with pancreatic cancer.Hepatobiliary Pancreat Dis Int. 2019 Aug;18(4):389-394. doi: 10.1016/j.hbpd.2019.06.004. Epub 2019 Jun 10. Hepatobiliary Pancreat Dis Int. 2019. PMID: 31230959
-
Rationale for en bloc vein resection in the treatment of pancreatic adenocarcinoma adherent to the superior mesenteric-portal vein confluence. Pancreatic Tumor Study Group.Ann Surg. 1996 Feb;223(2):154-62. doi: 10.1097/00000658-199602000-00007. Ann Surg. 1996. PMID: 8597509 Free PMC article.
-
Laparoscopic pancreaticoduodenectomy with portal or superior mesenteric vein resection and reconstruction for pancreatic cancer: A single-center experience.Hepatobiliary Pancreat Dis Int. 2023 Apr;22(2):147-153. doi: 10.1016/j.hbpd.2023.01.004. Epub 2023 Jan 18. Hepatobiliary Pancreat Dis Int. 2023. PMID: 36690522 Review.
-
Benefit from synchronous portal-superior mesenteric vein resection during pancreaticoduodenectomy for cancer: a meta-analysis.Eur J Surg Oncol. 2014 Apr;40(4):371-8. doi: 10.1016/j.ejso.2014.01.010. Epub 2014 Feb 7. Eur J Surg Oncol. 2014. PMID: 24560302 Review.
References
-
- Cai J, Chen H, Lu M, et al. Advances in the epidemiology of pancreatic cancer: Trends, risk factors, screening, and prognosis. Cancer Lett. 2021;520:1–11. - PubMed
-
- Kim SY, Fink MA, Perini M, et al. Age 80 years and over is not associated with increased morbidity and mortality following pancreaticoduodenectomy. ANZ J Surg. 2018;88:E445–50. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
