

Free-breathing myocardial T1 mapping using inversion-recovery radial FLASH and motion-resolved model-based reconstruction
- PMID: 36404631
- PMCID: PMC9892313
- DOI: 10.1002/mrm.29521
Free-breathing myocardial T1 mapping using inversion-recovery radial FLASH and motion-resolved model-based reconstruction
Abstract
Purpose: To develop a free-breathing myocardial mapping technique using inversion-recovery (IR) radial fast low-angle shot (FLASH) and calibrationless motion-resolved model-based reconstruction.
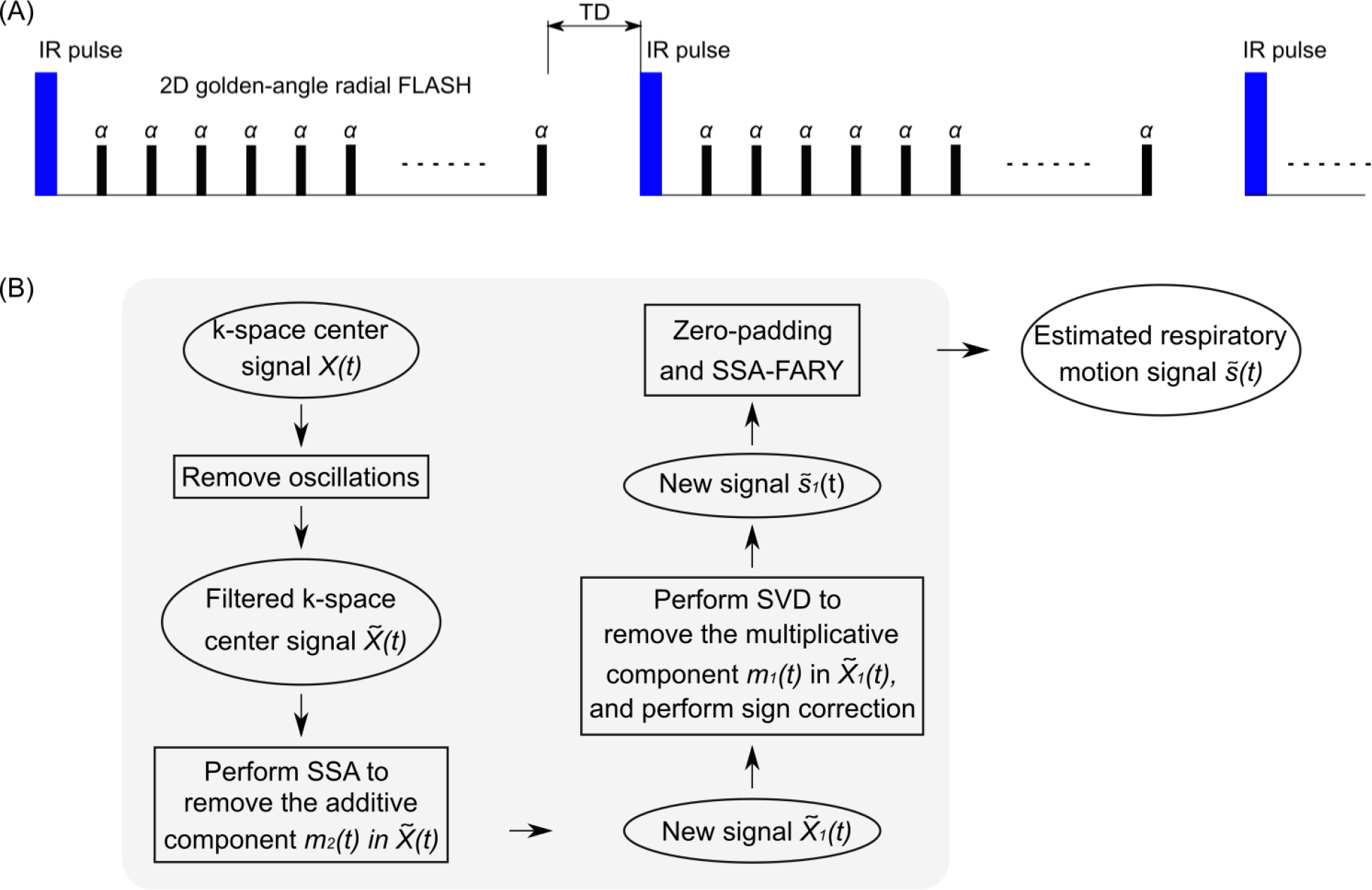
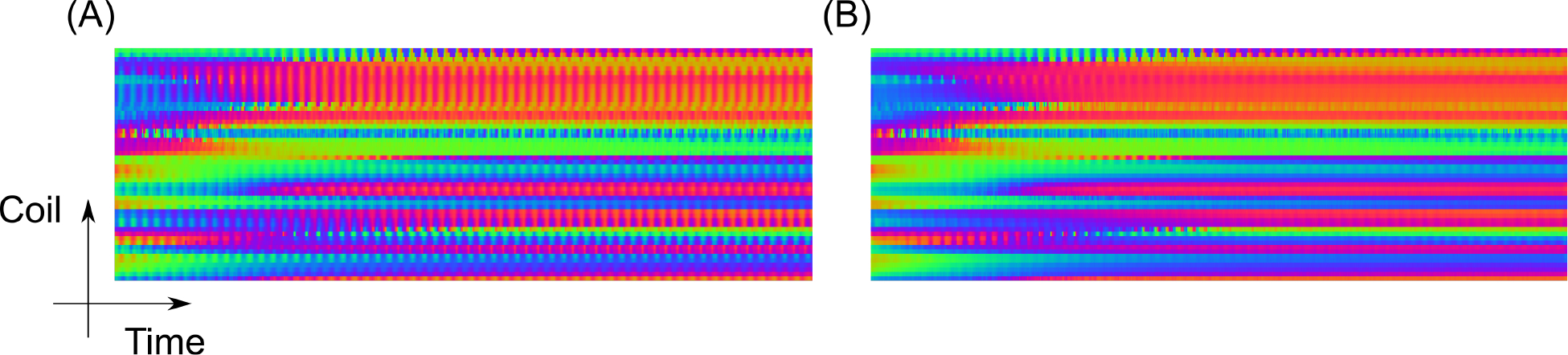
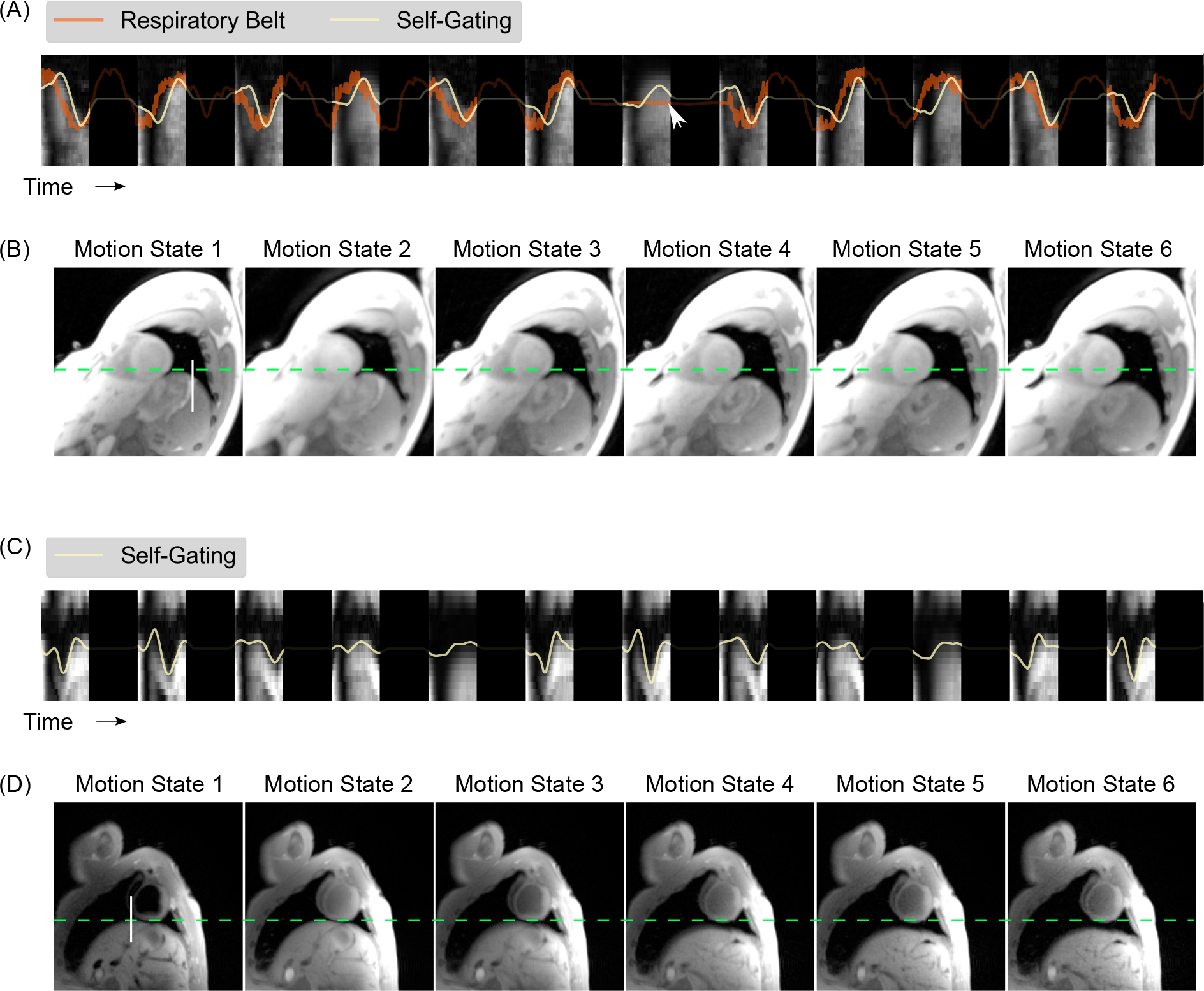
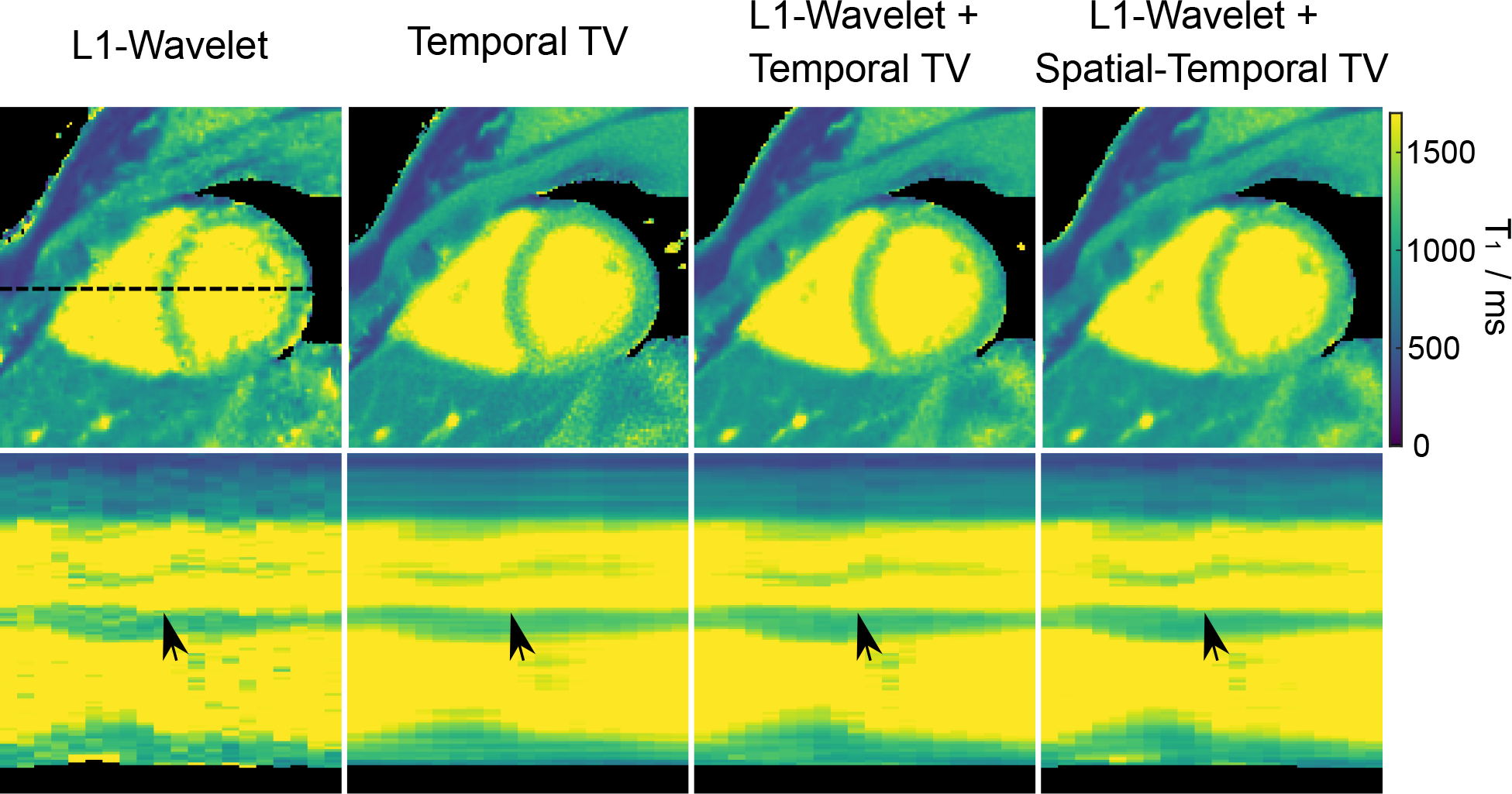
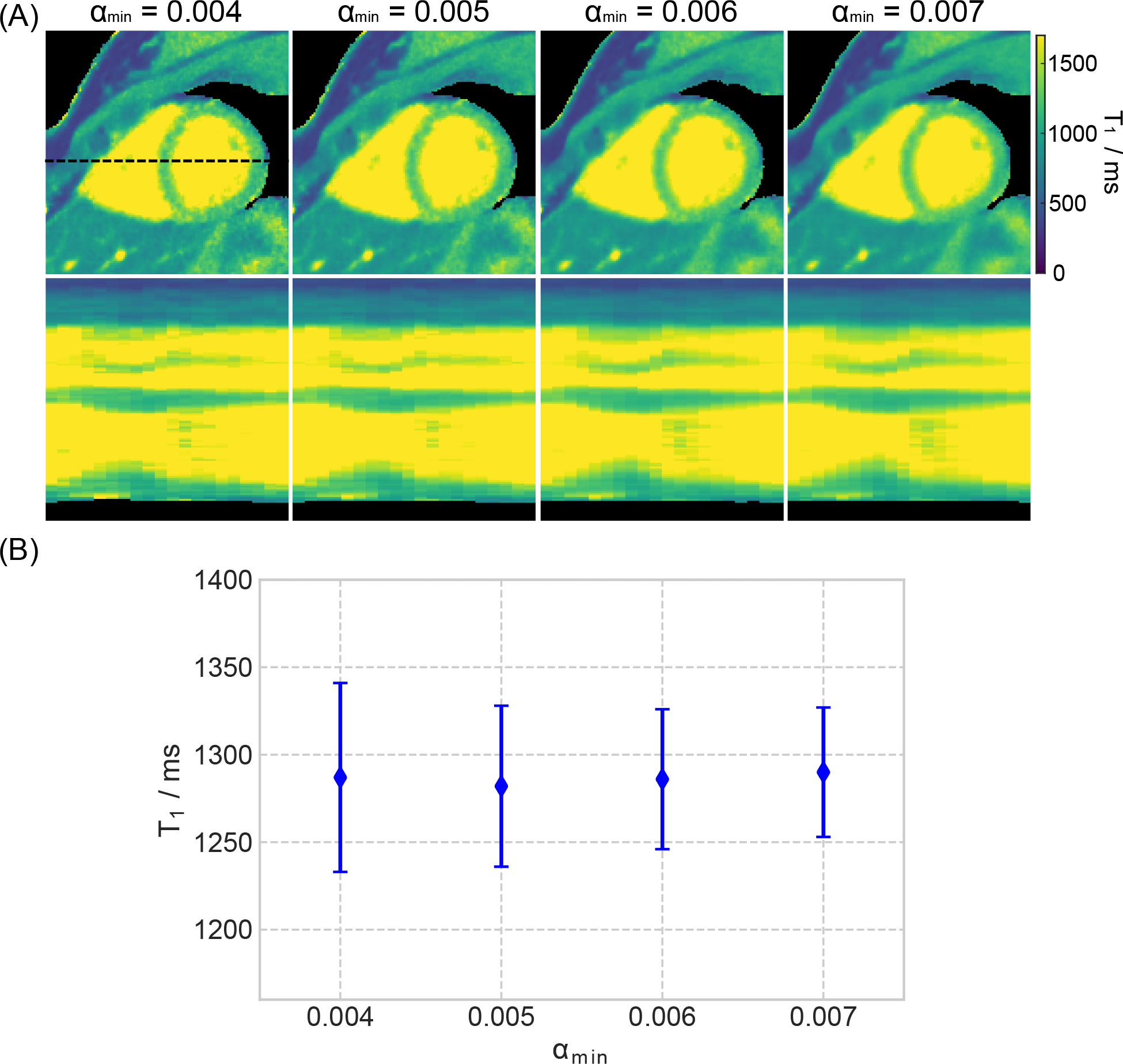
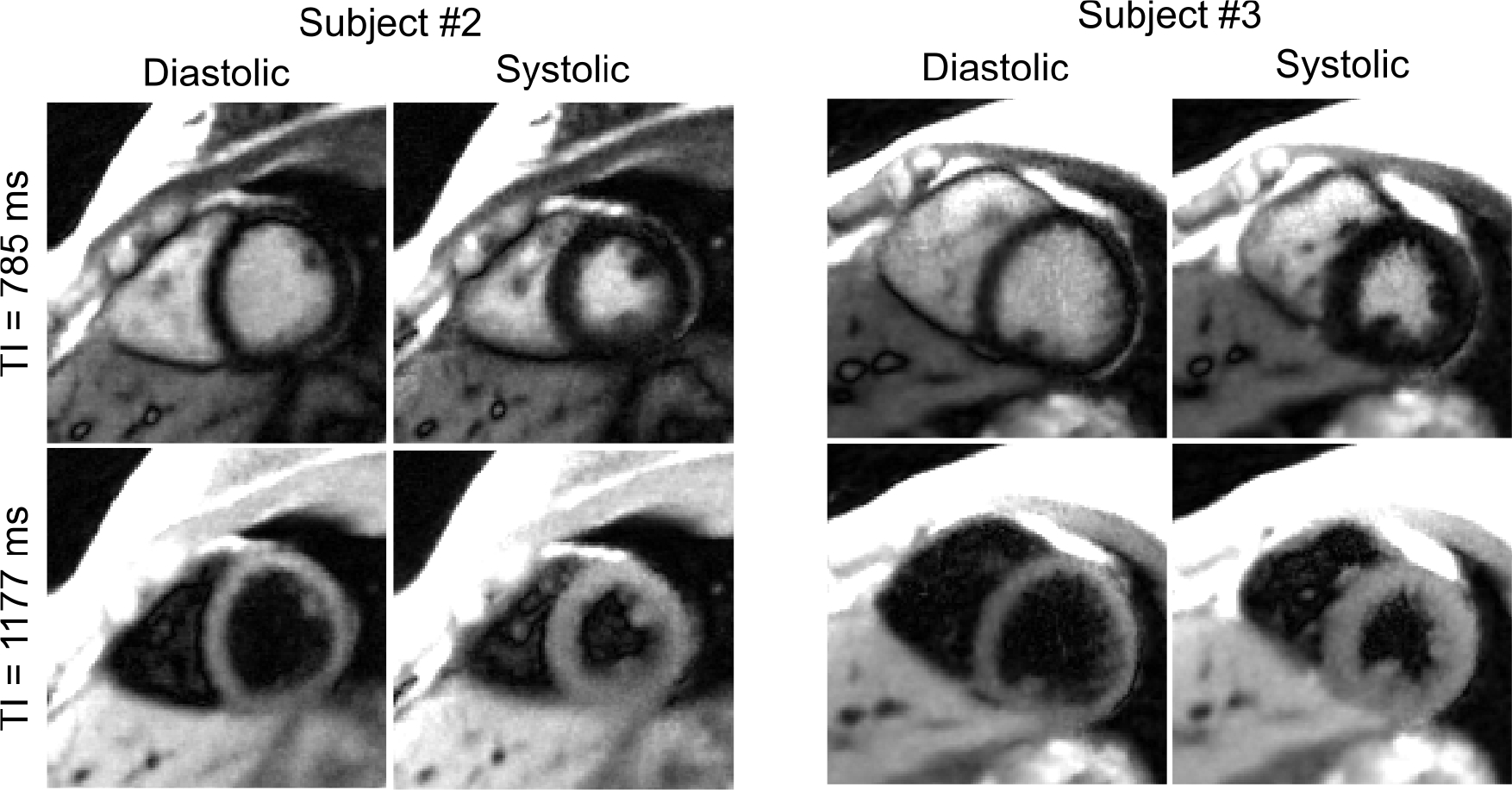
Methods: Free-running (free-breathing, retrospective cardiac gating) IR radial FLASH is used for data acquisition at 3T. First, to reduce the waiting time between inversions, an analytical formula is derived that takes the incomplete recovery into account for an accurate calculation. Second, the respiratory motion signal is estimated from the k-space center of the contrast varying acquisition using an adapted singular spectrum analysis (SSA-FARY) technique. Third, a motion-resolved model-based reconstruction is used to estimate both parameter and coil sensitivity maps directly from the sorted k-space data. Thus, spatiotemporal total variation, in addition to the spatial sparsity constraints, can be directly applied to the parameter maps. Validations are performed on an experimental phantom, 11 human subjects, and a young landrace pig with myocardial infarction.
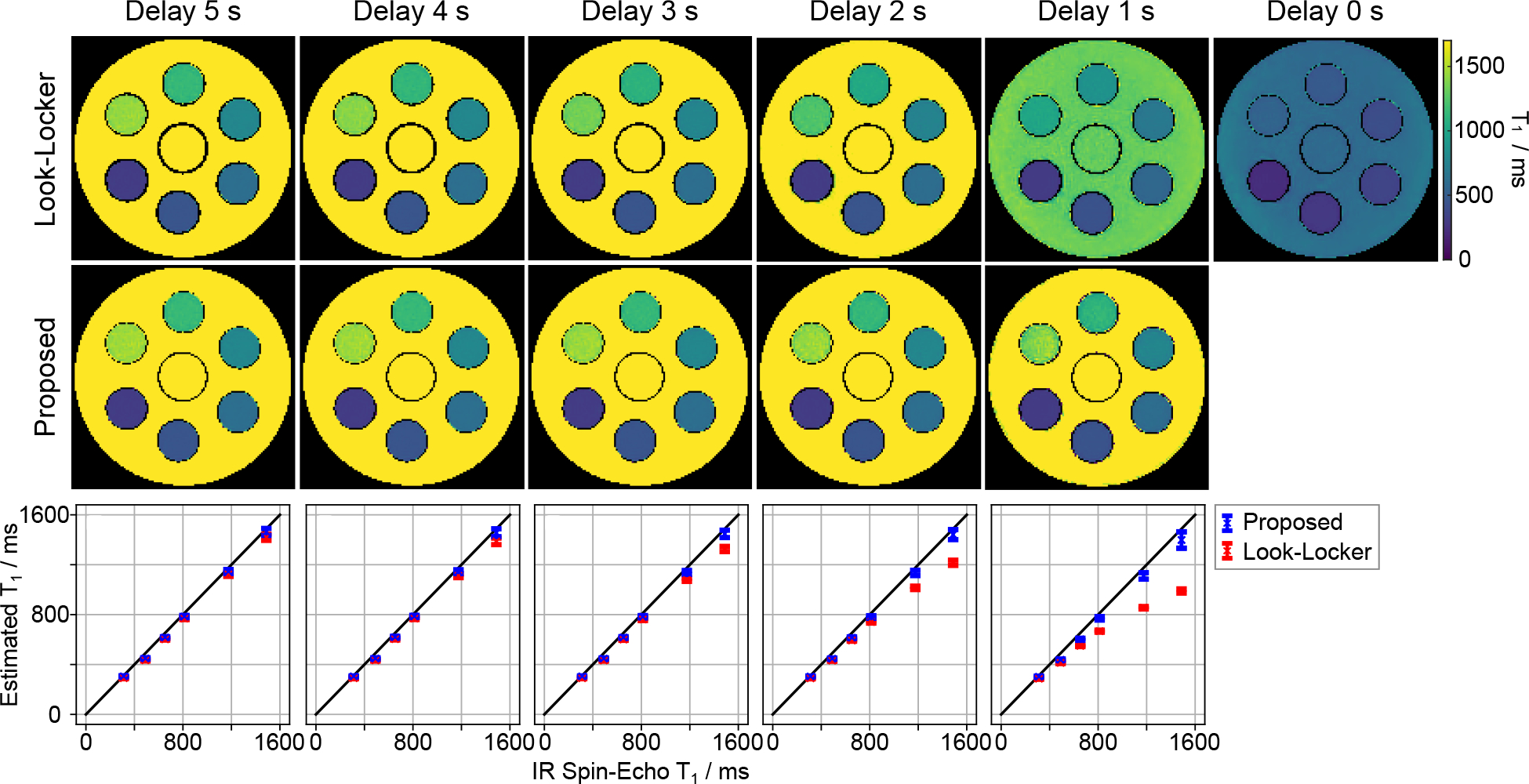
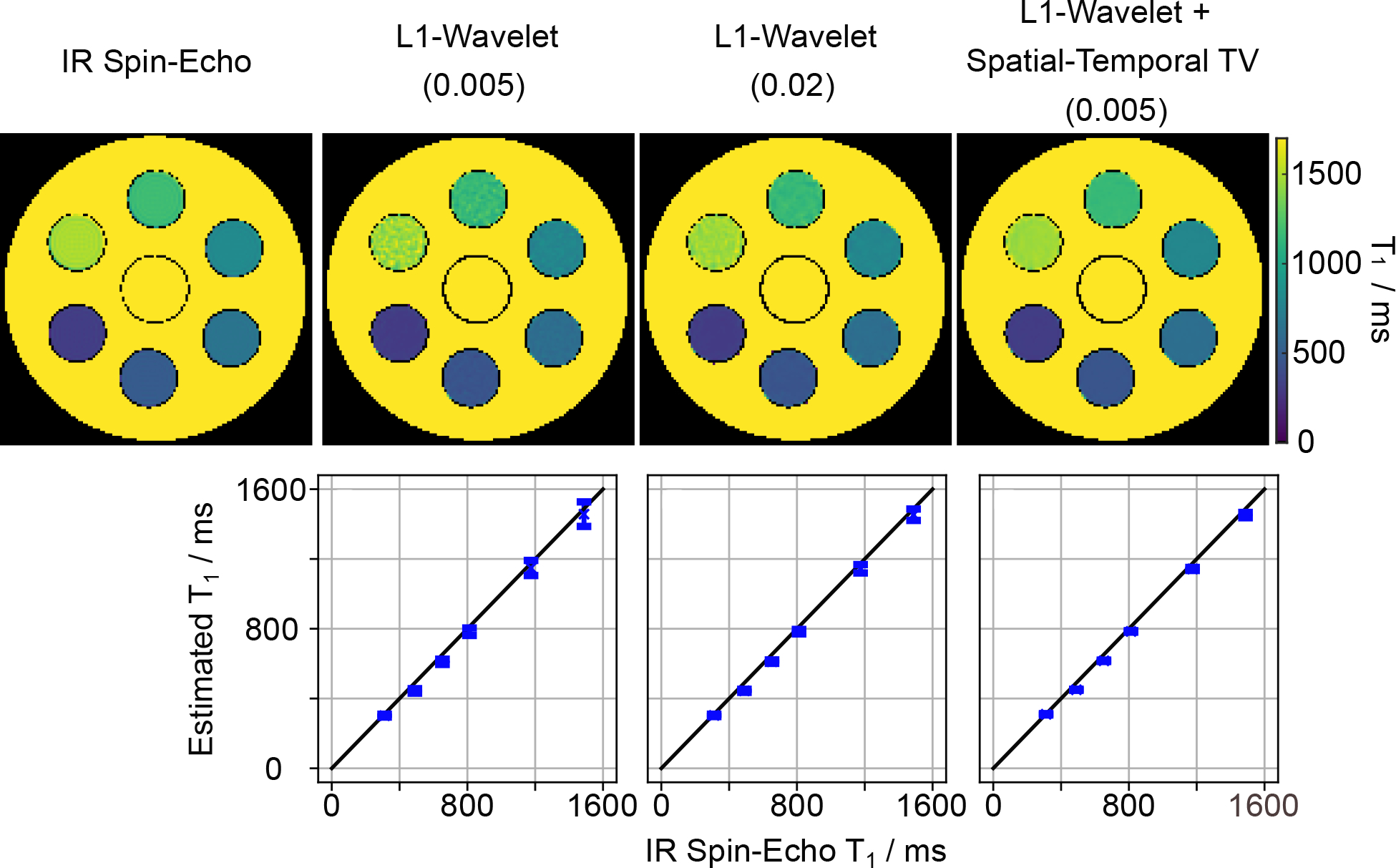
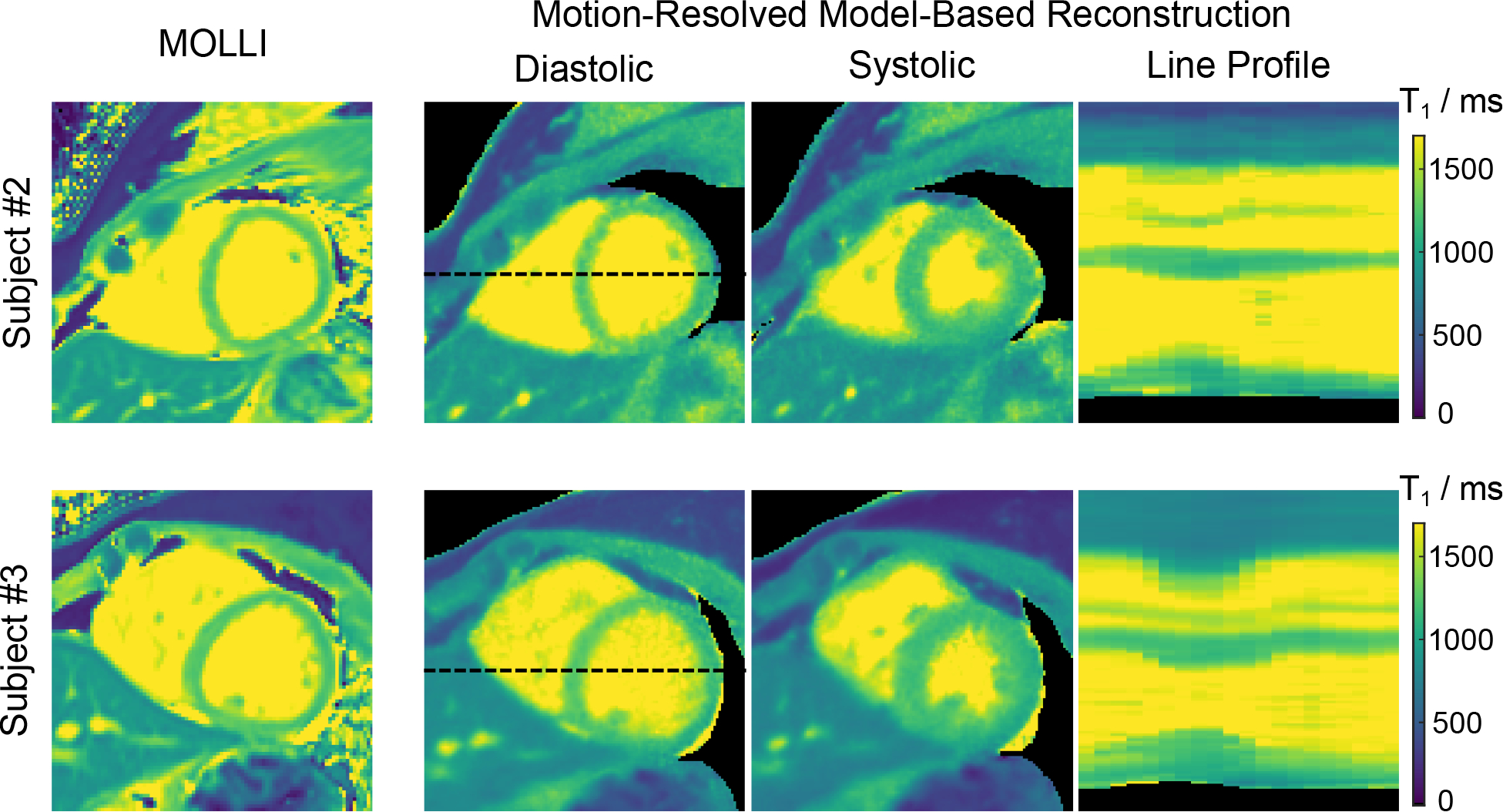
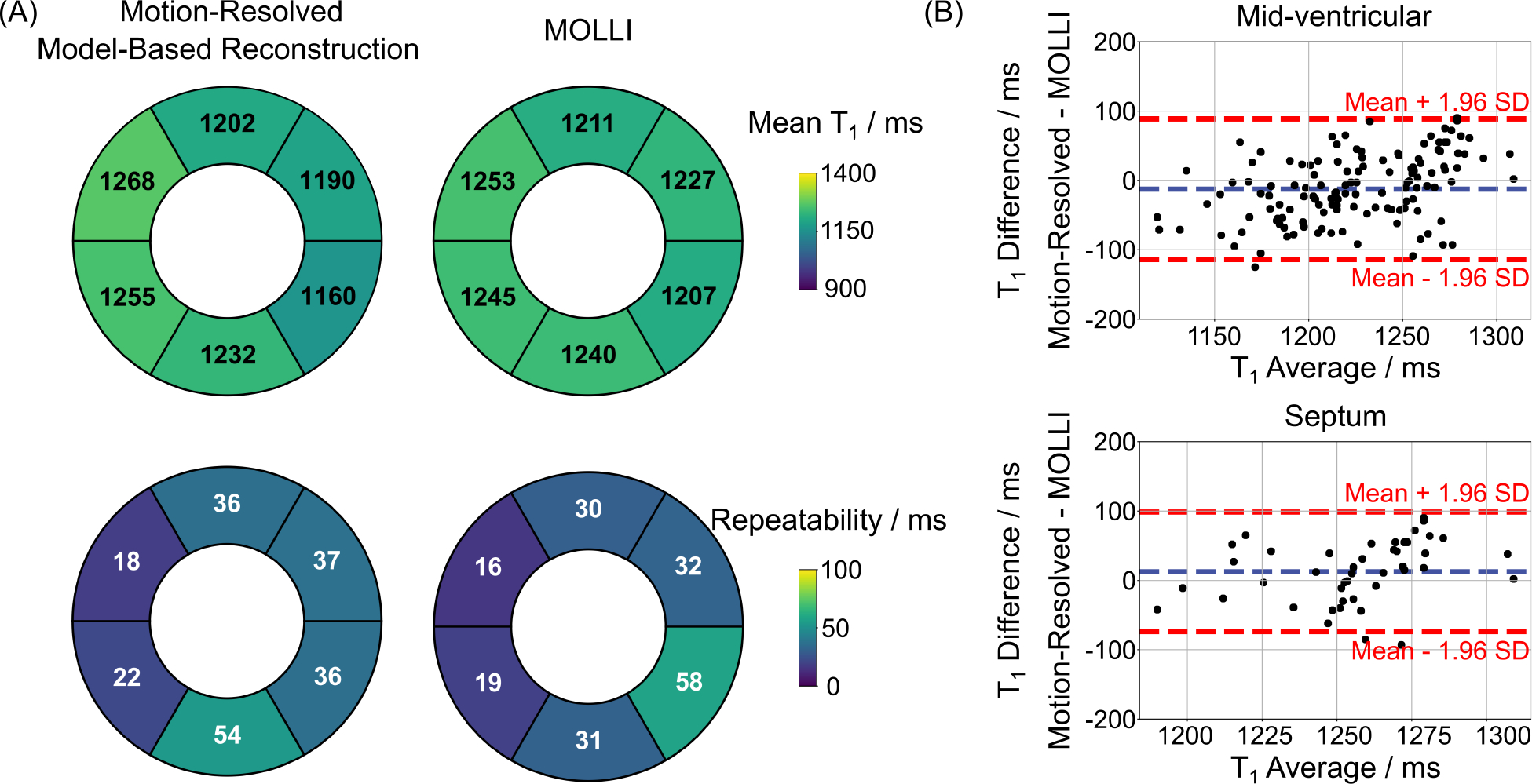
Results: In comparison to an IR spin-echo reference, phantom results confirm good accuracy, when reducing the waiting time from 5 s to 1 s using the new correction. The motion-resolved model-based reconstruction further improves precision compared to the spatial regularization-only reconstruction. Aside from showing that a reliable respiratory motion signal can be estimated using modified SSA-FARY, in vivo studies demonstrate that dynamic myocardial maps can be obtained within 2 min with good precision and repeatability.
Conclusion: Motion-resolved myocardial mapping during free-breathing with good accuracy, precision and repeatability can be achieved by combining inversion-recovery radial FLASH, self-gating and a calibrationless motion-resolved model-based reconstruction.
Keywords: free-breathing myocardial T1 mapping; motion-resolved model-based reconstruction; radial FLASH; self-gating; spatiotemporal total variation.
© 2022 The Authors. Magnetic Resonance in Medicine published by Wiley Periodicals LLC on behalf of International Society for Magnetic Resonance in Medicine.
Conflict of interest statement
Conflict of Interest
The authors declare no competing interests.
Figures
Similar articles
-
Model-based myocardial T1 mapping with sparsity constraints using single-shot inversion-recovery radial FLASH cardiovascular magnetic resonance.J Cardiovasc Magn Reson. 2019 Sep 19;21(1):60. doi: 10.1186/s12968-019-0570-3. J Cardiovasc Magn Reson. 2019. PMID: 31533736 Free PMC article.
-
Model-based reconstruction for simultaneous multi-slice mapping using single-shot inversion-recovery radial FLASH.Magn Reson Med. 2021 Mar;85(3):1258-1271. doi: 10.1002/mrm.28497. Epub 2020 Sep 16. Magn Reson Med. 2021. PMID: 32936487 Free PMC article.
-
Accelerated free-breathing liver fat and quantification using multi-echo stack-of-radial MRI with motion-resolved multidimensional regularized reconstruction: Initial retrospective evaluation.Magn Reson Med. 2024 Sep;92(3):1149-1161. doi: 10.1002/mrm.30117. Epub 2024 Apr 22. Magn Reson Med. 2024. PMID: 38650444
-
Free-breathing high isotropic resolution quantitative susceptibility mapping (QSM) of liver using 3D multi-echo UTE cones acquisition and respiratory motion-resolved image reconstruction.Magn Reson Med. 2023 Nov;90(5):1844-1858. doi: 10.1002/mrm.29779. Epub 2023 Jul 1. Magn Reson Med. 2023. PMID: 37392413 Free PMC article.
-
Free-Running Cardiac and Respiratory Motion-Resolved Imaging: A Paradigm Shift for Managing Motion in Cardiac MRI?Diagnostics (Basel). 2024 Sep 3;14(17):1946. doi: 10.3390/diagnostics14171946. Diagnostics (Basel). 2024. PMID: 39272732 Free PMC article. Review.
Cited by
-
Rapid, High-resolution and Distortion-free Mapping of Fetal Brain using Multi-echo Radial FLASH and Model-based Reconstruction.ArXiv [Preprint]. 2025 May 27:arXiv:2501.00256v4. ArXiv. 2025. Update in: Magn Reson Med. 2025 Jun 18. doi: 10.1002/mrm.30604. PMID: 39801623 Free PMC article. Updated. Preprint.
-
Pilot tone-based prospective correction of respiratory motion for free-breathing myocardial T1 mapping.MAGMA. 2023 Feb;36(1):135-150. doi: 10.1007/s10334-022-01032-4. Epub 2022 Aug 3. MAGMA. 2023. PMID: 35921020 Free PMC article.
-
Free-breathing 3D cardiac extracellular volume (ECV) mapping using a linear tangent space alignment (LTSA) model.Magn Reson Med. 2025 Feb;93(2):536-549. doi: 10.1002/mrm.30284. Epub 2024 Oct 14. Magn Reson Med. 2025. PMID: 39402014
-
B0 navigator enables respiratory motion navigation in radial stack-of-stars liver Look-Locker T1 mapping.Magn Reson Med. 2025 Oct;94(4):1458-1468. doi: 10.1002/mrm.30567. Epub 2025 May 20. Magn Reson Med. 2025. PMID: 40395015 Free PMC article.
-
Accelerated Cartesian cardiac T2 mapping based on a calibrationless locally low-rank tensor constraint.Quant Imaging Med Surg. 2024 Oct 1;14(10):7654-7670. doi: 10.21037/qims-24-740. Epub 2024 Sep 26. Quant Imaging Med Surg. 2024. PMID: 39429619 Free PMC article.
References
-
- Moon JC, Messroghli DR, Kellman P, Piechnik SK, Robson MD, Ugander M, Gatehouse PD, Arai AE, Friedrich MG, Neubauer S et al. Myocardial T1 mapping and extracellular volume quantification: a Society for Cardiovascular Magnetic Resonance (SCMR) and CMR Working Group of the European Society of Cardiology consensus statement. J. Cardiovasc. Magn. Reson. 2013; 15:92. - PMC - PubMed
-
- Puntmann VO, Voigt T, Chen Z, Mayr M, Karim R, Rhode K, Pastor A, CarrWhite G, Razavi R, Schaeffter T et al. Native T1 mapping in differentiation of normal myocardium from diffuse disease in hypertrophic and dilated cardiomyopathy. JACC: Cardiovascular Imaging 2013; 6:475–484. - PubMed
-
- Messroghli DR, Radjenovic A, Kozerke S, Higgins DM, Sivananthan MU, Ridgway JP. Modified Look-Locker Inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magn. Reson. Med. 2004; 52:141–146. - PubMed
-
- Chow K, Flewitt JA, Green JD, Pagano JJ, Friedrich MG, Thompson RB. Saturation recovery single-shot acquisition (SASHA) for myocardial T1 mapping. Magn. Reson. Med. 2014; 71:2082–2095. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
