

Breast Cancer Screening: Is There Room for De-escalation?
- PMID: 36404936
- PMCID: PMC9640864
- DOI: 10.1007/s12609-022-00465-z
Breast Cancer Screening: Is There Room for De-escalation?
Abstract
Purpose of review: Breast cancer screening is highly controversial and different agencies have widely varying guidelines. Yet it is currently used extensively in the USA and frequently the thought is "the more, the better." The purpose of this review is to objectively assess the risks and benefits of screening mammography and consider whether there may be areas where it could be de-escalated.
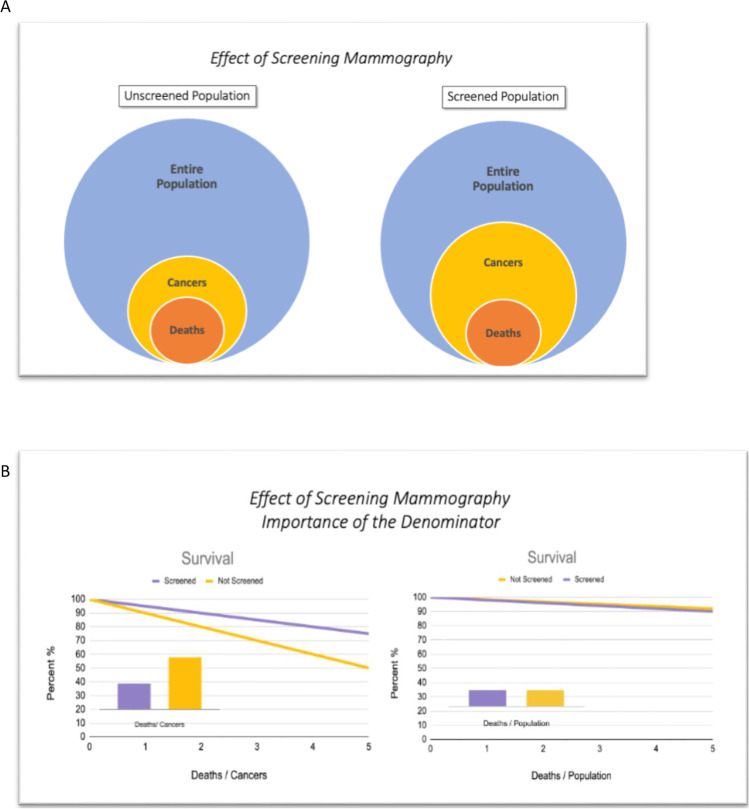
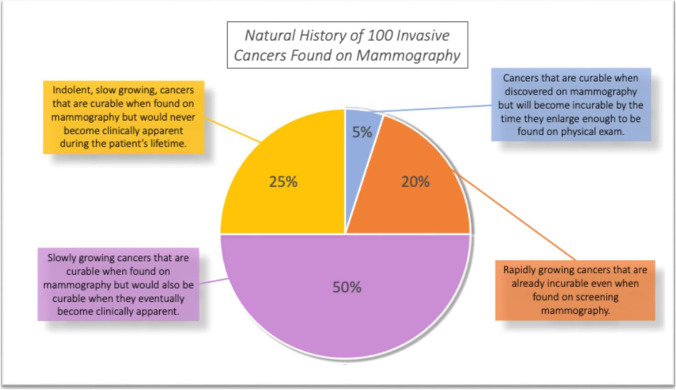
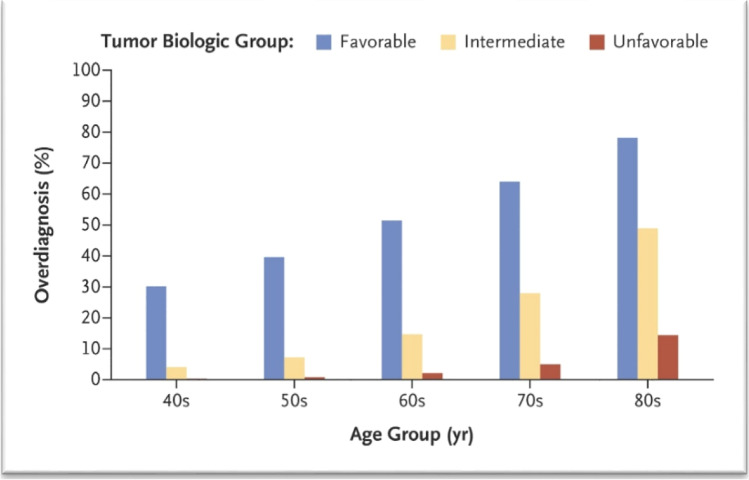
Recent findings: Over the past few years, there have been several meta-analyses that are concordant, and it is now agreed that the main benefit of screening mammography is about a 20% reduction in breast cancer mortality. This actually benefits about 5% of patients with mammographically detected tumors. We now appreciate that the main harm of screening is overdiagnosis, i.e. detection of a cancer that will not cause the patient any harm and would not have ever been detected without the screening. This currently represents about 20 to 30% of screening detected cancers. Finding extra cancers with more intense screening is not always good, because in this situation, the risk of overdiagnosis increases and the benefit decreases. In some groups, the risk of overdiagnosis approaches 75%.
Summary: Our goal should be not only to find more cancers, but to avoid finding cancers that would never have caused the patient any harm and lead to unnecessary treatment. The authors suggest some situations where it may be reasonable to de-escalate screening.
Keywords: Breast cancer screening; De-escalation of breast cancer screening; Harms of breast cancer screening; Overdiagnosis.
© The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature 2022, Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Conflict of interest statement
Conflict of InterestThe authors declare no competing interests.
Figures
References
-
- Breast Cancer Statistics | How common is breast cancer? https://www.cancer.org/cancer/breast-cancer/about/how-common-is-breast-c.... Accessed 4/1/2022.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous