

Acute myocardial infarction in a patient with congenitally corrected transposition of the great arteries and complex coronary anatomy-a case report
- PMID: 36405539
- PMCID: PMC9668067
- DOI: 10.1093/ehjcr/ytac423
Acute myocardial infarction in a patient with congenitally corrected transposition of the great arteries and complex coronary anatomy-a case report
Abstract
Background: Congenitally corrected transposition of the great arteries (ccTGA) is a rare congenital heart anomaly with atrioventricular and ventriculoarterial discordance that is often associated with other cardiac and coronary artery anomalies. Here, we report a case of a patient with ccTGA and non-ST elevation myocardial infarction (NSTEMI) with challenging coronary anatomy that was treated with stress-perfusion cardiac magnetic resonance imaging (spCMR) guided percutaneous coronary intervention (PCI).
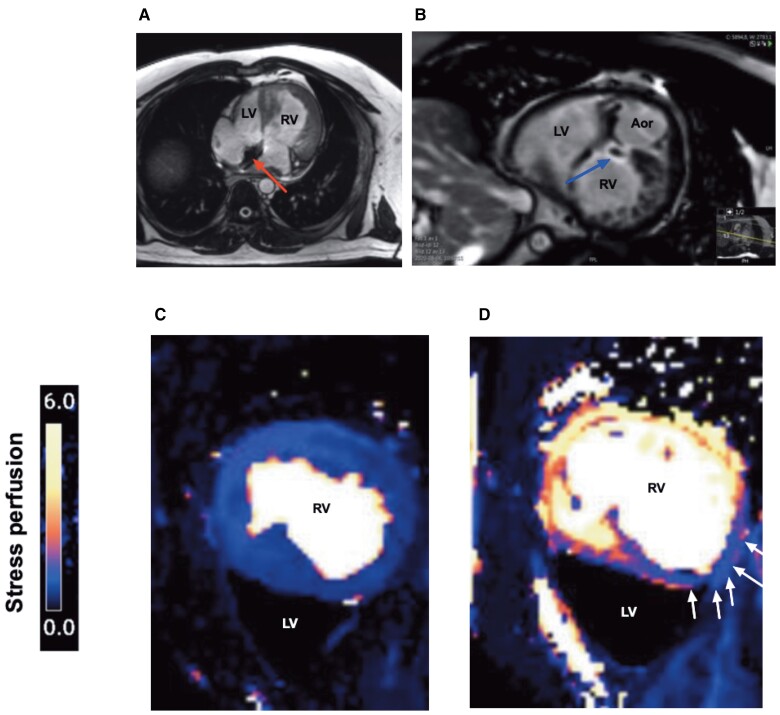
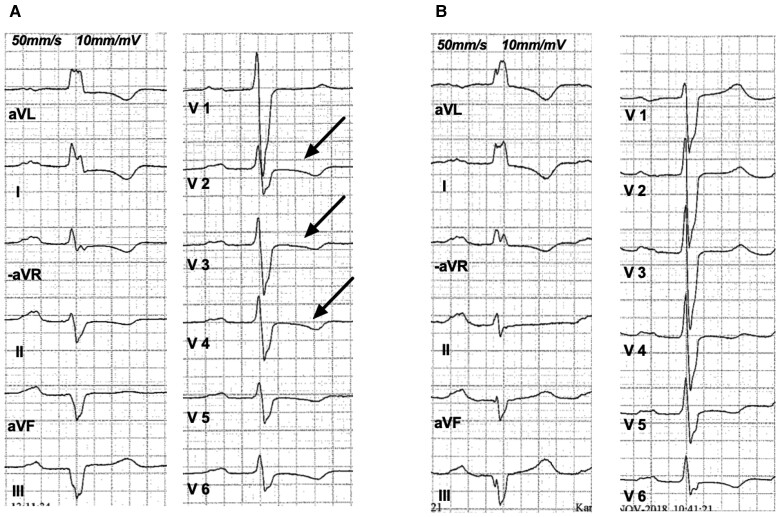
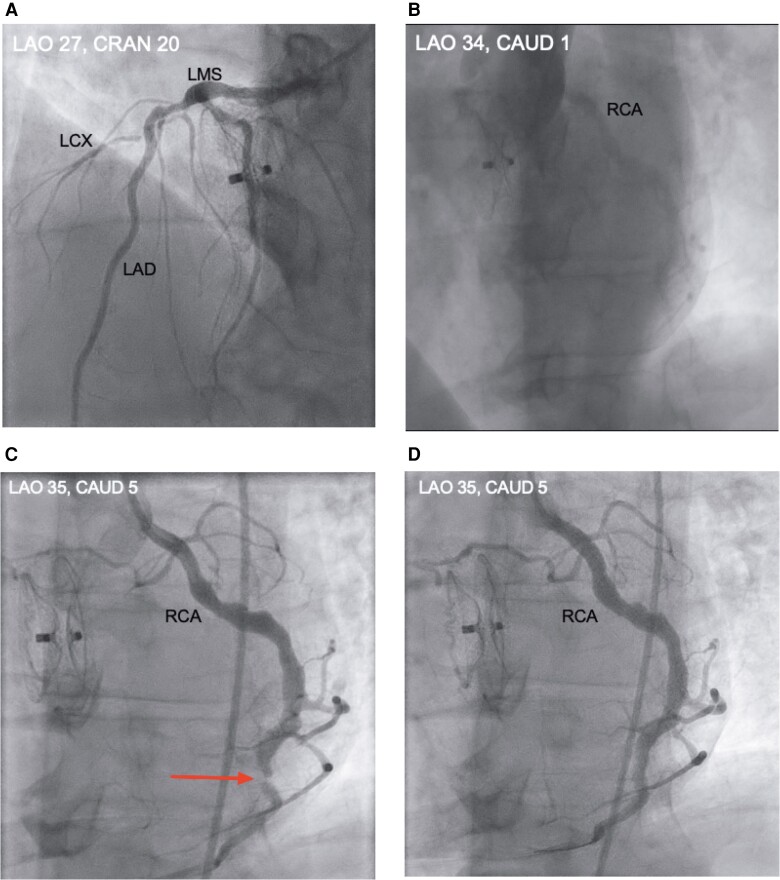
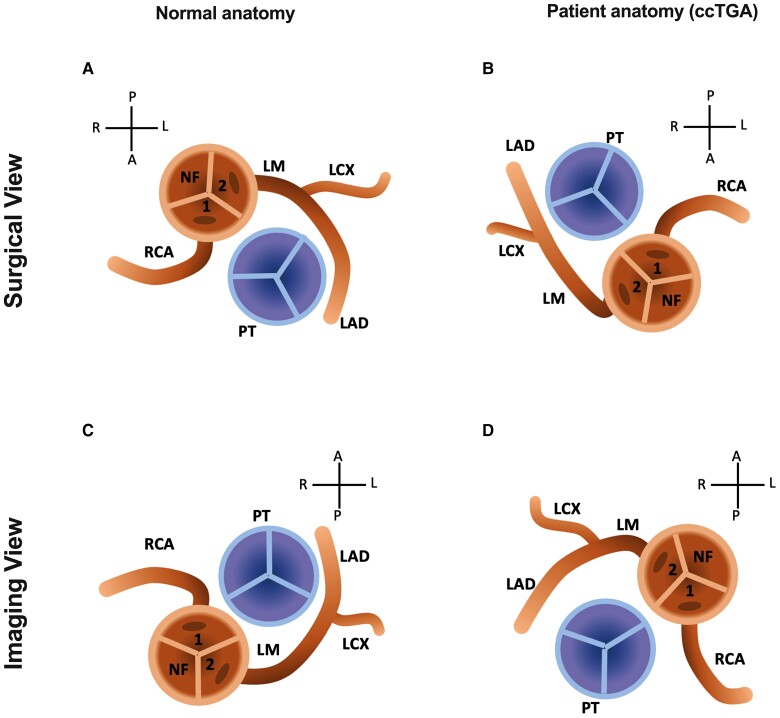
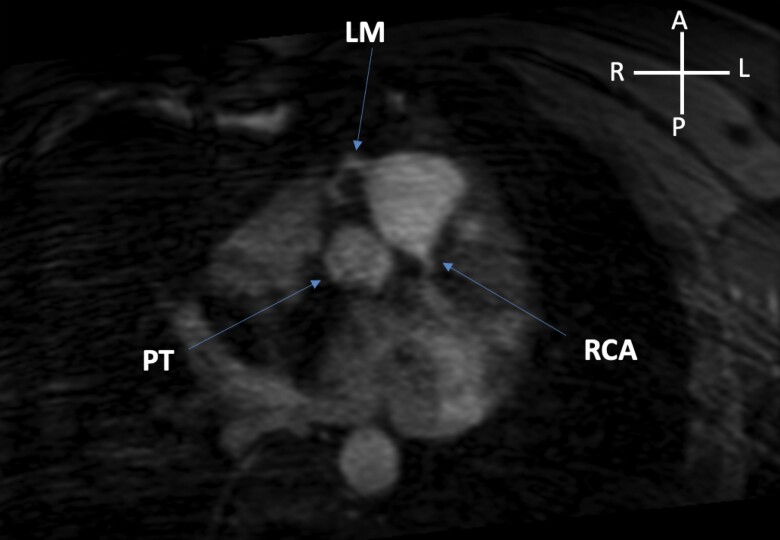
Case summary: A 46-year-old male smoker with ccTGA, dyslipidaemia, diabetes Type 2 managed with dietary restrictions and a family history of premature myocardial infarction, presented with typical chest pain, elevated cardiac troponin levels and ECG-changes indicative of ischaemia. The patient was diagnosed with NSTEMI and underwent initial urgent coronary angiography (CA) without apparent significant stenosis, although the right coronary artery (RCA) could not be selectively investigated. The patient had coronary anatomy 1R-2LCX according to the Leiden convention, which is the usual anatomy in patients with ccTGA. Despite this, CA was challenging due to the different anatomy compared with individuals with normally positioned great vessels. The patient remained highly symptomatic with chest pain at moderate exertion. To improve identification of the anatomic location and extent of ischaemia, we performed spCMR with adenosine. This revealed a limited septal infarction (likely embolic) in the right ventricle and reversible ischaemia in two inferior right ventricular segments. A second angiography, selectively investigating RCA demonstrated a significant stenosis in the distal RCA that was successfully treated with a drug-eluting stent. Fractional flow reserve (FFR) measurements of the left coronary arteries demonstrated hemodynamically non-significant stenosis. The patient's symptoms resolved, and he remained asymptomatic at one month follow-up.
Discussion: This ccTGA patient had multiple risk factors for coronary artery disease and presented with NSTEMI. Diagnosis and treatment were challenging due to complex cardiac anatomy and associated different origins of the coronary arteries. We highlight the importance of careful evaluation of the coronary anatomy and functional testing using for example spCMR and FFR to target the culprit coronary vessel(s) in ccTGA complicated by NSTEMI.
Keywords: Acute myocardial infarction; Case report; Congenitally corrected transposition of the great arteries; Coronary artery anomalies.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: Fahd Asaad: None to declare. Peder Sörensson: Honoraria and consultant fees (Pfizer). Andreas Rück: Research grants to our institution (Boston Scientific). Consulting fees (Boston Scientific). Consulting, proctoring fees (Boston Scientific). Advisory Board (Boston Scientific). Edit Nagy: None to declare. Juliane Jurga: None to declare. Marcus Ståhlberg: None to declare..
Figures
Similar articles
-
Congenitally corrected transposition of the great arteries and coronary artery disease: a case report in an 83-year-old male.Eur Heart J Case Rep. 2025 May 7;9(5):ytaf161. doi: 10.1093/ehjcr/ytaf161. eCollection 2025 May. Eur Heart J Case Rep. 2025. PMID: 40336940 Free PMC article.
-
Congenitally corrected transposition of the great arteries: is it really a transposition? An anatomical study of the right ventricular septal surface.J Anat. 2020 Feb;236(2):325-333. doi: 10.1111/joa.13097. Epub 2019 Oct 27. J Anat. 2020. PMID: 31657020 Free PMC article.
-
Nature Decides Survival: Primary Angioplasty in Congenitally Corrected Transposition of Great Arteries at 76 Years of Age.JACC Case Rep. 2019 Dec 18;1(5):705-710. doi: 10.1016/j.jaccas.2019.10.026. eCollection 2019 Dec 18. JACC Case Rep. 2019. PMID: 34316914 Free PMC article.
-
Congenitally corrected transposition of the great arteries and concomitant coronary artery and valvular disease in the adult patient.Congenit Heart Dis. 2010 Nov-Dec;5(6):629-34. doi: 10.1111/j.1747-0803.2009.00360.x. Congenit Heart Dis. 2010. PMID: 21106026 Review.
-
A great imitator in adult cardiology practice: congenitally corrected transposition of the great arteries.Congenit Heart Dis. 2017 Mar;12(2):143-152. doi: 10.1111/chd.12453. Epub 2017 Feb 22. Congenit Heart Dis. 2017. PMID: 28225206 Review.
Cited by
-
Congenitally corrected transposition of the great arteries and coronary artery disease: a case report in an 83-year-old male.Eur Heart J Case Rep. 2025 May 7;9(5):ytaf161. doi: 10.1093/ehjcr/ytaf161. eCollection 2025 May. Eur Heart J Case Rep. 2025. PMID: 40336940 Free PMC article.
References
-
- Mah K, Friedberg MK. Congenitally corrected transposition of the great arteries: situs solitus or inversus. Circ Cardiovasc Imaging 2014;7:849–851. - PubMed
-
- Baumgartner H, De Backer J. The ESC clinical practice guidelines for the management of adult congenital heart disease 2020. Eur Heart J 2020;41:4153–4154. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous