

Lyme borreliosis in pregnancy and associations with parent and offspring health outcomes: An international cross-sectional survey
- PMID: 36405612
- PMCID: PMC9669415
- DOI: 10.3389/fmed.2022.1022766
Lyme borreliosis in pregnancy and associations with parent and offspring health outcomes: An international cross-sectional survey
Abstract
Background: Lyme disease (LD) is a complex tick-borne pathology caused by Borrelia burgdorferi sensu lato bacteria. Currently, there are limited data regarding the health outcomes of people infected during pregnancy, the potential for perinatal transmission to their fetus, and the long-term effects on these children. Therefore, the primary objective of this survey study was to investigate the impact of LD in pregnancy on both the parent and their offspring.
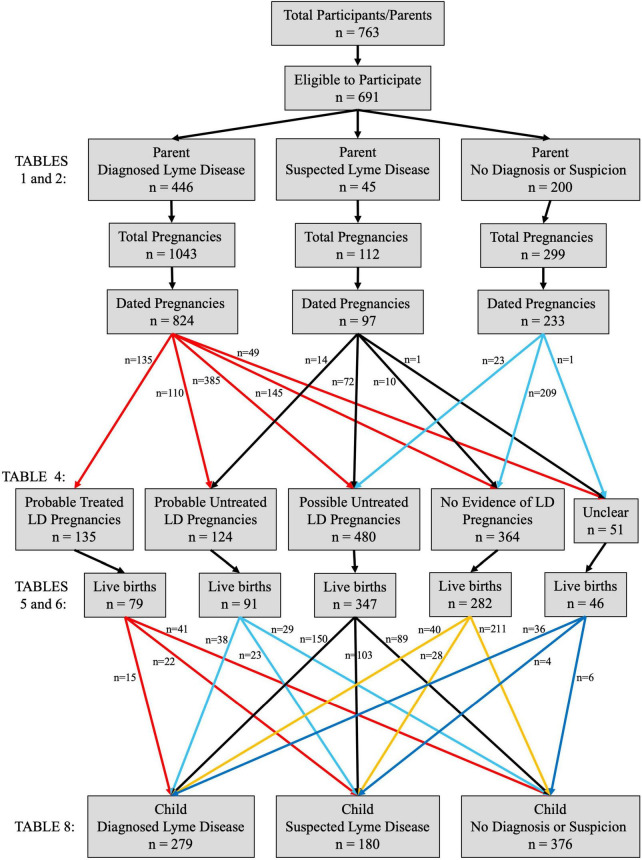
Methods: A seven-section survey was developed and administered in REDCap. Although recruitment was primarily through LD-focused organizations, participation was open to anyone over the age of 18 who had been pregnant. Participant health/symptoms were compared across those with "Diagnosed LD," "Suspected LD," or "No LD" at any time in their lives. The timing of LD events in the participants' histories (tick bite, diagnosis, treatment start, etc.) were then utilized to classify the participants' pregnancies into one of five groups: "Probable Treated LD," "Probable Untreated LD," "Possible Untreated LD," "No Evidence of LD," and "Unclear."
Results: A total of 691 eligible people participated in the survey, of whom 65% had Diagnosed LD, 6% had Suspected LD, and 29% had No LD ever. Both the Diagnosed LD and Suspected LD groups indicated a high symptom burden (p < 0.01). Unfortunately, direct testing of fetal/newborn tissues for Borrelia burgdorferi only occurred following 3% of pregnancies at risk of transmission; positive/equivocal results were obtained in 14% of these cases. Pregnancies with No Evidence of LD experienced the fewest complications (p < 0.01) and were most likely to result in a live birth (p = 0.01) and limited short- and long-term offspring pathologies (p < 0.01). Within the LD-affected pregnancy groups, obtaining treatment did not decrease complications for the parent themselves but did ameliorate neonatal health status, with reduced rates of rashes, hypotonia, and respiratory distress (all p < 0.01). The impact of parent LD treatment on longer-term child outcomes was less clear.
Conclusion: Overall, this pioneering survey represents significant progress toward understanding the effects of LD on pregnancy and child health. A large prospective study of pregnant people with LD, combining consistent diagnostic testing, exhaustive assessment of fetal/newborn samples, and long-term offspring follow-up, is warranted.
Keywords: Lyme borreliosis; Lyme disease; birth outcomes; child health; pregnancy; survey; symptoms; transmission.
Copyright © 2022 Leavey, MacKenzie, Faber, Lloyd, Mao, Wills, Boucoiran, Cates, Omar, Marquez and Darling.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A systematic review on the impact of gestational Lyme disease in humans on the fetus and newborn.PLoS One. 2018 Nov 12;13(11):e0207067. doi: 10.1371/journal.pone.0207067. eCollection 2018. PLoS One. 2018. PMID: 30419059 Free PMC article.
-
Committee Opinion No. 399: Management of Tick Bites and Lyme Disease During Pregnancy.J Obstet Gynaecol Can. 2020 May;42(5):644-653. doi: 10.1016/j.jogc.2020.01.001. J Obstet Gynaecol Can. 2020. PMID: 32414479
-
Polymerase chain reaction in diagnosis of Borrelia burgdorferi infections and studies on taxonomic classification.APMIS Suppl. 2002;(105):1-40. APMIS Suppl. 2002. PMID: 11985118
-
The evolving story of Borrelia burgdorferi sensu lato transmission in Europe.Parasitol Res. 2022 Mar;121(3):781-803. doi: 10.1007/s00436-022-07445-3. Epub 2022 Feb 5. Parasitol Res. 2022. PMID: 35122516 Free PMC article. Review.
-
Isolation of live Borrelia burgdorferi sensu lato spirochaetes from patients with undefined disorders and symptoms not typical for Lyme borreliosis.Clin Microbiol Infect. 2016 Mar;22(3):267.e9-15. doi: 10.1016/j.cmi.2015.11.009. Epub 2015 Dec 8. Clin Microbiol Infect. 2016. PMID: 26673735
Cited by
-
An Unusual Case of Serologically Confirmed Post-Partum Lyme Disease Following an Asymptomatic Borrelia burgdorferi Infection Acquired during Pregnancy and Lacking Vertical Transmission in Utero.Pathogens. 2024 Feb 20;13(3):186. doi: 10.3390/pathogens13030186. Pathogens. 2024. PMID: 38535530 Free PMC article.
-
Developing a Prospective Gestational Lyme Disease Study.Methods Mol Biol. 2024;2742:259-278. doi: 10.1007/978-1-0716-3561-2_18. Methods Mol Biol. 2024. PMID: 38165628
-
Examining Infant and Child Neurodevelopmental Outcomes After Lyme Disease During Pregnancy.Pathogens. 2024 Nov 22;13(12):1029. doi: 10.3390/pathogens13121029. Pathogens. 2024. PMID: 39770289 Free PMC article. Review.
-
Vector-borne infectious diseases in pregnancy in the era of climate change: A focus on mosquito- and tick-borne pathogens (Review).Exp Ther Med. 2025 Jul 21;30(3):174. doi: 10.3892/etm.2025.12924. eCollection 2025 Sep. Exp Ther Med. 2025. PMID: 40746445 Free PMC article. Review.
-
Perinatal transmission of Lyme disease: A qualitative study investigating the research priorities of patients with Lyme disease in pregnancy.PLoS One. 2024 Feb 6;19(2):e0294265. doi: 10.1371/journal.pone.0294265. eCollection 2024. PLoS One. 2024. PMID: 38319904 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials