

Sugammadex to Facilitate Neurologic Assessment in Severely Brain-Injured Patients: A Retrospective Analysis and Practical Guidance
- PMID: 36407180
- PMCID: PMC9673186
- DOI: 10.7759/cureus.30466
Sugammadex to Facilitate Neurologic Assessment in Severely Brain-Injured Patients: A Retrospective Analysis and Practical Guidance
Abstract
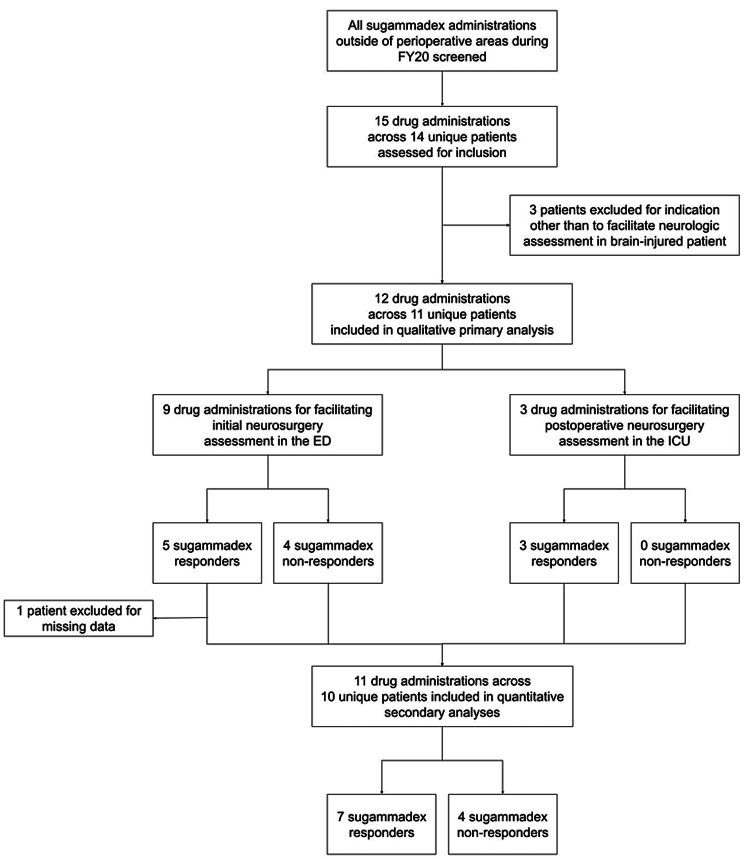
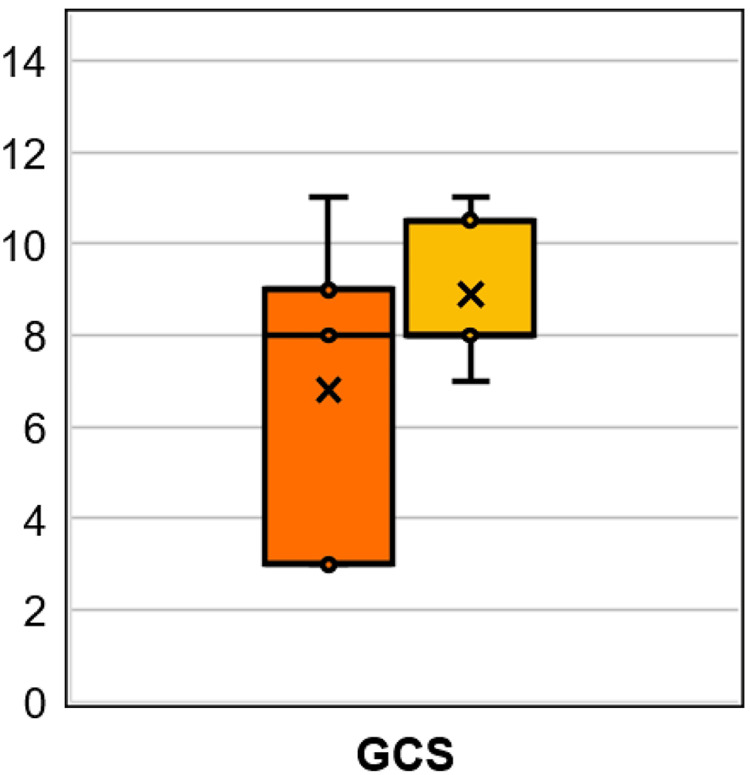
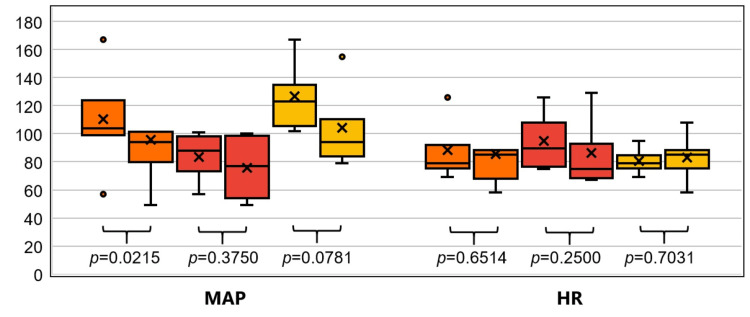
Background Widely used in anesthetic management, sugammadex is increasingly employed in the reversal of neuromuscular blocking agents (NMBAs) in the emergency department and critical care arena, where little evaluative data currently exists. This study explored the utility and safety of using sugammadex to facilitate neurologic assessments in critically ill, NMBA-exposed patients. Methods We pursued a retrospective case series and single-arm cohort analysis of all brain-injured patients receiving sugammadex to facilitate neurologic evaluation during one year at a high-volume Level 1 trauma center. The primary outcome was the qualitative impact of sugammadex administration on neurosurgeon decision-making. Secondary outcomes included the change to Glasgow Coma Scale (GCS) and hemodynamic parameters compared before and after sugammadex administration. Sugammadex dosing was also assessed across various weight scalars to explore dose-response trends and generate preliminary guidance for use in this setting. Results Our study criteria yielded 12 sugammadex administrations across 11 patients, the majority of whom had sustained a traumatic brain injury. All sugammadex administrations were adjudicated as beneficial to neurosurgeon decision-making and 50% were associated with a change to prognosis and plan. Sugammadex was associated with an increase in the GCS of 1-8 points among the 67% of patients who responded. Mean arterial pressure decreased significantly after sugammadex administration (median 94 vs. 104 mmHg, p=0.0215, median change of -8 mmHg [95%CI -25-3 mmHg]). No apparent dose-response trends were observed for changes to GCS or hemodynamic parameters. Conclusions The use of sugammadex to facilitate neurologic assessment after NMBA exposure in brain-injured patients was frequently associated with clinically meaningful changes to the neurologic exam and treatment plan. The risks of hemodynamic compromise and care complexity should be collaboratively weighed before pursuing this modality. An empiric sugammadex dose of 200 mg appears reasonable for this purpose, but further evaluation of NMBA reversal in the neurocritically ill outside of procedural settings is warranted.
Keywords: emergency neurosurgery; intracranial hemorrhage; neurologic assessment; neuromuscular blockade; neuroprognostication; non-depolarizing neuromuscular blocking agents; rapid sequence intubation; rocuronium; sugammadex; traumatic brain injury.
Copyright © 2022, Hyland et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Utility of neuromuscular blockade reversal in the evaluation of acute neurosurgical patients: A retrospective case-series.J Clin Neurosci. 2022 Oct;104:82-87. doi: 10.1016/j.jocn.2022.08.009. Epub 2022 Aug 16. J Clin Neurosci. 2022. PMID: 35981464
-
Sugammadex Efficacy and Dosing for Rocuronium Reversal Outside of Perioperative Settings.Hosp Pharm. 2023 Apr;58(2):194-199. doi: 10.1177/00185787221126682. Epub 2022 Sep 29. Hosp Pharm. 2023. PMID: 36890961 Free PMC article.
-
Use and Outcomes of Sugammadex for Neurological Examination after Neuromuscular Blockade in the Emergency Department.West J Emerg Med. 2025 Mar;26(2):347-352. doi: 10.5811/westjem.29328. West J Emerg Med. 2025. PMID: 40145930 Free PMC article.
-
What is the Role of Sugammadex in the Emergency Department?J Emerg Med. 2021 Jan;60(1):44-53. doi: 10.1016/j.jemermed.2020.08.006. Epub 2020 Sep 19. J Emerg Med. 2021. PMID: 32962903 Review.
-
Sugammadex, the first selective relaxant binding agent for neuromuscular block reversal.Drugs Today (Barc). 2012 Jun;48(6):405-13. doi: 10.1358/dot.2012.48.6.1813474. Drugs Today (Barc). 2012. PMID: 22745926 Review.
Cited by
-
Skeletal Muscle Relaxants and Their Impact on Intracranial Pressure in Neurosurgery.Med Sci Monit. 2025 Jan 3;31:e946569. doi: 10.12659/MSM.946569. Med Sci Monit. 2025. PMID: 39748489 Free PMC article. Review.
-
The effect of neuromuscular blocking reversal agents on perioperative neurocognitive function after general anaesthesia: a systematic review and meta-analysis.BMC Anesthesiol. 2025 Apr 4;25(1):152. doi: 10.1186/s12871-025-03019-9. BMC Anesthesiol. 2025. PMID: 40186115 Free PMC article.
References
-
- Guidelines on muscle relaxants and reversal in anaesthesia. Plaud B, Baillard C, Bourgain JL, et al. Anaesth Crit Care Pain Med. 2020;39:125–142. - PubMed
-
- Current status of neuromuscular reversal and monitoring: challenges and opportunities. Brull SJ, Kopman AF. Anesthesiology. 2017;126:173–190. - PubMed
-
- Sugammadex: A review of neuromuscular blockade reversal. Keating GM. Drugs. 2016;76:1041–1052. - PubMed
-
- Conceptual and technical insights into the basis of neuromuscular monitoring. Naguib M, Brull SJ, Johnson KB. Anaesthesia. 2017;72 Suppl 1:16–37. - PubMed
LinkOut - more resources
Full Text Sources