

Prediction, prevention, and management of right ventricular failure after left ventricular assist device implantation: A comprehensive review
- PMID: 36407460
- PMCID: PMC9671519
- DOI: 10.3389/fcvm.2022.1040251
Prediction, prevention, and management of right ventricular failure after left ventricular assist device implantation: A comprehensive review
Abstract
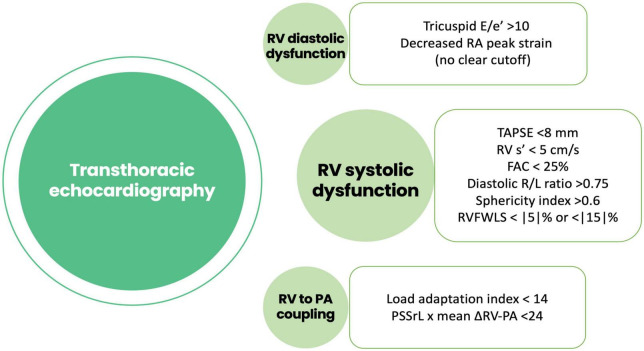
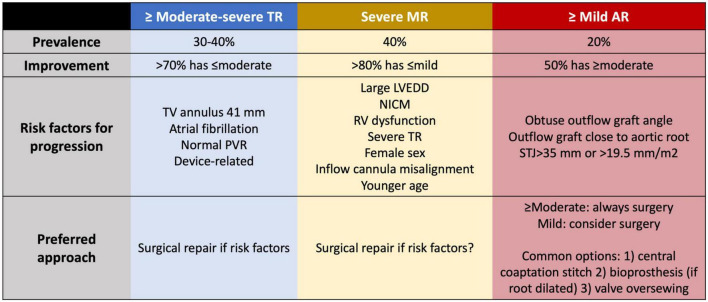
Left ventricular assist devices (LVADs) are increasingly common across the heart failure population. Right ventricular failure (RVF) is a feared complication that can occur in the early post-operative phase or during the outpatient follow-up. Multiple tools are available to the clinician to carefully estimate the individual risk of developing RVF after LVAD implantation. This review will provide a comprehensive overview of available tools for RVF prognostication, including patient-specific and right ventricle (RV)-specific echocardiographic and hemodynamic parameters, to provide guidance in patient selection during LVAD candidacy. We also offer a multidisciplinary approach to the management of early RVF, including indications and management of right ventricular assist devices in this setting to provide tools that help managing the failing RV.
Keywords: heart failure (HF); hemocompatibility adverse events (HRAE); left ventricular assist device (LVAD); right ventricle (RV); right ventricular assist device (RVAD); right ventricular failure (RVF).
Copyright © 2022 Rodenas-Alesina, Brahmbhatt, Rao, Salvatori and Billia.
Conflict of interest statement
ER-A has received non-conditioned grants from Biotronik, Microport, Johnson and Johnson, and Sanofi outside of the submitted work. DB has received travel support from Abbott and Biotronik, and honoraria, travel support and a grant from Boston Scientific outside of the submitted work. FB has received support from Abbott Laboratories for investigations outside of the submitted work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





Similar articles
-
Pre-operative atrial fibrillation and early right ventricular failure after left ventricular assist device implantation: a systematic review and meta-analysis.Am Heart J. 2021 Sep;239:120-128. doi: 10.1016/j.ahj.2021.05.009. Epub 2021 May 24. Am Heart J. 2021. PMID: 34038705
-
Left ventricular vs. biventricular mechanical support: Decision making and strategies for avoidance of right heart failure after left ventricular assist device implantation.Int J Cardiol. 2015 Nov 1;198:241-50. doi: 10.1016/j.ijcard.2015.06.103. Epub 2015 Jul 2. Int J Cardiol. 2015. PMID: 26232775 Review.
-
Pulmonary artery pulsatility index predicts right ventricular failure after left ventricular assist device implantation.J Heart Lung Transplant. 2016 Jan;35(1):67-73. doi: 10.1016/j.healun.2015.06.009. Epub 2015 Jun 17. J Heart Lung Transplant. 2016. PMID: 26212656
-
Right Ventricular Failure After Left Ventricular Assist Device Placement-The Beginning of the End or Just Another Challenge?J Cardiothorac Vasc Anesth. 2019 Apr;33(4):1105-1121. doi: 10.1053/j.jvca.2018.07.047. Epub 2018 Aug 7. J Cardiothorac Vasc Anesth. 2019. PMID: 30197170 Review.
-
The Right Ventricular Function After Left Ventricular Assist Device (RVF-LVAD) study: rationale and preliminary results.Eur Heart J Cardiovasc Imaging. 2016 Apr;17(4):429-37. doi: 10.1093/ehjci/jev162. Epub 2015 Jul 9. Eur Heart J Cardiovasc Imaging. 2016. PMID: 26160395 Free PMC article. Clinical Trial.
Cited by
-
Impact of early CVP monitoring on 1-year mortality in patients with congestive heart failure in the ICU: a retrospective analysis based on the MIMIC-IV2.2 database.BMC Cardiovasc Disord. 2025 Mar 7;25(1):162. doi: 10.1186/s12872-025-04602-1. BMC Cardiovasc Disord. 2025. PMID: 40055591 Free PMC article.
-
Advancing intraoperative assessment of the right ventricle through three-dimensional transesophageal echocardiography.Can J Anaesth. 2023 Oct;70(10):1549-1559. doi: 10.1007/s12630-023-02562-8. Epub 2023 Sep 26. Can J Anaesth. 2023. PMID: 37752377 English. No abstract available.
-
The Prognostic Role of Pulmonary Arterial Elastance in Patients Undergoing Left Ventricular Assist Device Implantation: A Pilot Study.J Clin Med. 2024 Nov 24;13(23):7102. doi: 10.3390/jcm13237102. J Clin Med. 2024. PMID: 39685561 Free PMC article.
-
Right heart failure after left ventricular assist device implantation: latest insights and knowledge gaps on mechanism and prediction.Front Cardiovasc Med. 2025 May 22;12:1586389. doi: 10.3389/fcvm.2025.1586389. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40476140 Free PMC article. Review.
-
The association of right ventricular function with outcomes after cardiac surgery: a systematic review.Can J Anaesth. 2025 Feb;72(2):285-318. doi: 10.1007/s12630-024-02898-9. Epub 2025 Feb 12. Can J Anaesth. 2025. PMID: 39939498 English.
References
-
- Goldstein DJ, Meyns B, Xie R, Cowger J, Pettit S, Nakatani T, et al. Third annual report from the ISHLT mechanically assisted circulatory support registry: a comparison of centrifugal and axial continuous-flow left ventricular assist devices. J Heart Lung Transplant. (2019) 38:352–63. 10.1016/j.healun.2019.02.004 - DOI - PubMed
-
- Frankfurter C, Molinero M, Vishram-Nielsen JKK, Foroutan F, Mak S, Rao V, et al. Predicting the risk of right ventricular failure in patients undergoing left ventricular assist device implantation: a systematic review. Circ Heart Fail. (2020) 13:e006994. 10.1161/CIRCHEARTFAILURE.120.006994 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous