

Dietary metal intake and the prevalence of erectile dysfunction in US men: Results from National Health and Nutrition Examination Survey 2001-2004
- PMID: 36407550
- PMCID: PMC9668876
- DOI: 10.3389/fnut.2022.974443
Dietary metal intake and the prevalence of erectile dysfunction in US men: Results from National Health and Nutrition Examination Survey 2001-2004
Abstract
Background: Erectile dysfunction (ED) mainly affects men over 40 years of age and is a common clinical condition. In addition to hypertension and diabetes, environment, and lifestyle are also significantly associated with erectile dysfunction. The relationship between dietary trace metal intake and ED has not been studied.
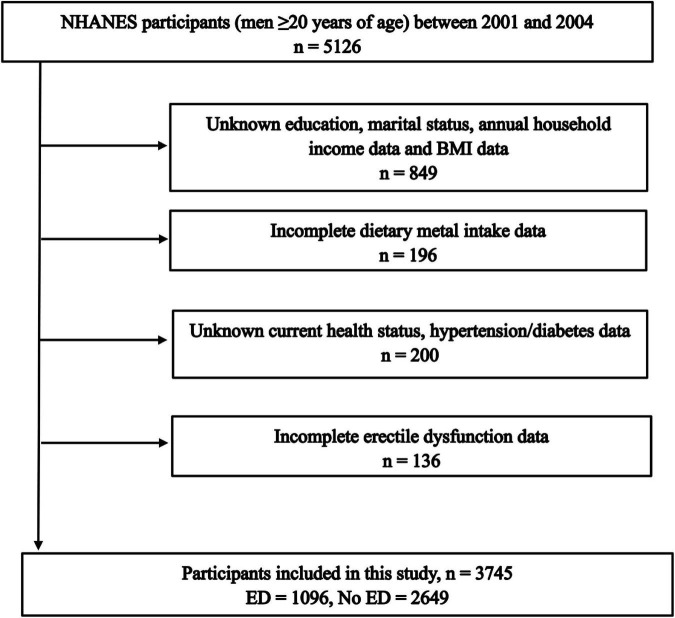
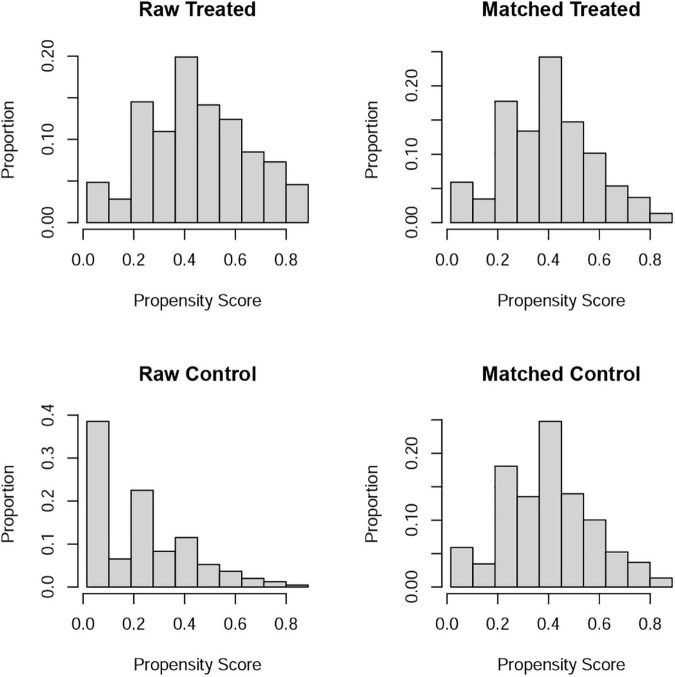
Materials and methods: Data on participants were obtained from the National Health and Nutrition Examination Survey for this study, and those with incomplete information on clinical variables were excluded. Dose-response curve analysis was used to investigate the relationship between dietary trace metal intake and ED prevalence. Multivariate logistic regression analysis was used to adjust for confounders to further investigate the relationship between dietary trace metal intake and ED prevalence. 1:1 propensity score matching (PSM) was performed to adjust for differences between clinical variables for data reanalysis to confirm the reliability of the results.
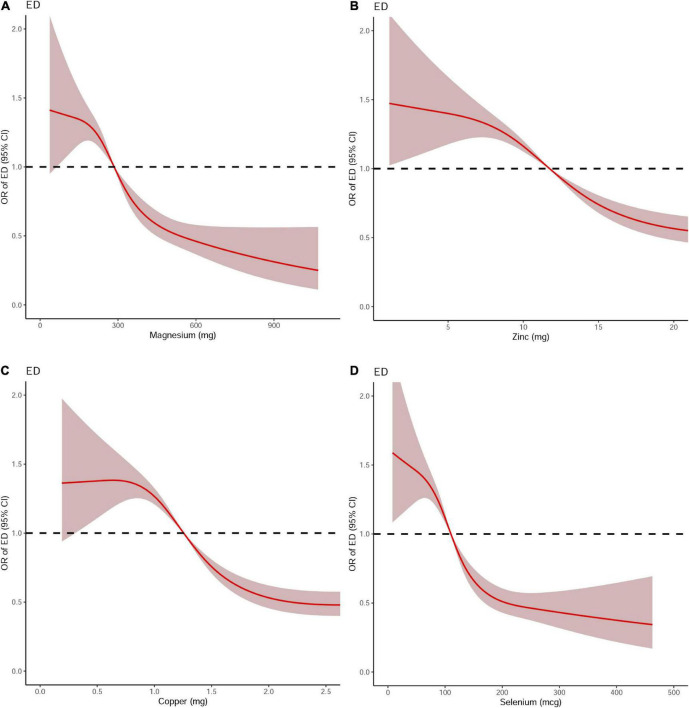
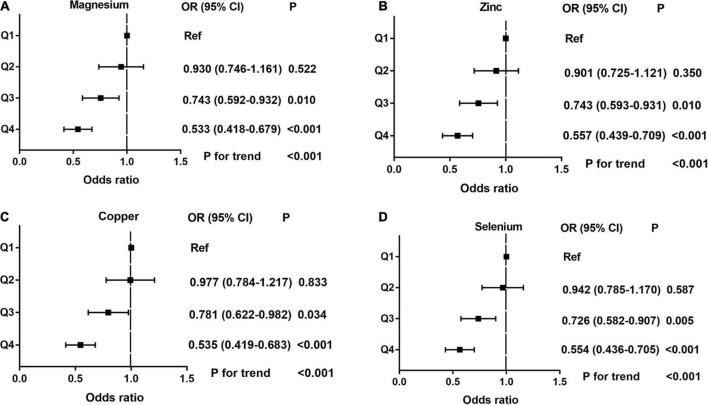
Results: A total of 3,745 individuals were included in the study, including 1096 ED patients and 2,649 participants without ED. Dietary intake of trace metals (Mg, Zn, Cu, and Se) was significantly higher in participants without ED than in ED patients (all P < 0.001). Dose-response curve analysis showed a significant negative association between these dietary metal intakes and ED prevalence (all P < 0.001). Multivariate logistic regression analysis adjusted for confounders (age, education, BMI, annual household income, hypertension, diabetes, marital status, race, and current health status) revealed that increased dietary metal intake reduced the odds ratio of ED. 1:1 PSM reanalysis further confirmed the validity of the results.
Conclusion: Increasing dietary intake of trace metals (magnesium, zinc, copper, and selenium) within the upper limit is beneficial in reducing the prevalence of ED.
Keywords: National Health and Nutrition Examination Survey (NHANES); atherosclerosis; dietary trace metals intake; erectile dysfunction; nutrition.
Copyright © 2022 Liu, Li, Xu, Yu, Mao, Sun, Xu and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Consensus development conference statement. National institutes of health. Impotence. Int J Impot Res. (1993) 5:181–284. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous