

Left ventricle chest compression improves ETCO2, blood pressure, and cerebral blood velocity in a swine model of cardiac arrest and cardiopulmonary resuscitation
- PMID: 36407570
- PMCID: PMC9672447
- DOI: 10.1016/j.resplu.2022.100326
Left ventricle chest compression improves ETCO2, blood pressure, and cerebral blood velocity in a swine model of cardiac arrest and cardiopulmonary resuscitation
Abstract
Introduction: During cardiopulmonary resuscitation (CPR), high quality chest compressions are critical to organ perfusion, especially the brain. Yet, the optimal location for chest compressions is unclear. It was hypothesized that compared with the standard chest compression (SCC) location, left ventricle chest compressions (LVCCs) would result in greater ETCO2, blood pressure (BP), and cerebral blood velocity (CBV) during CPR in swine.
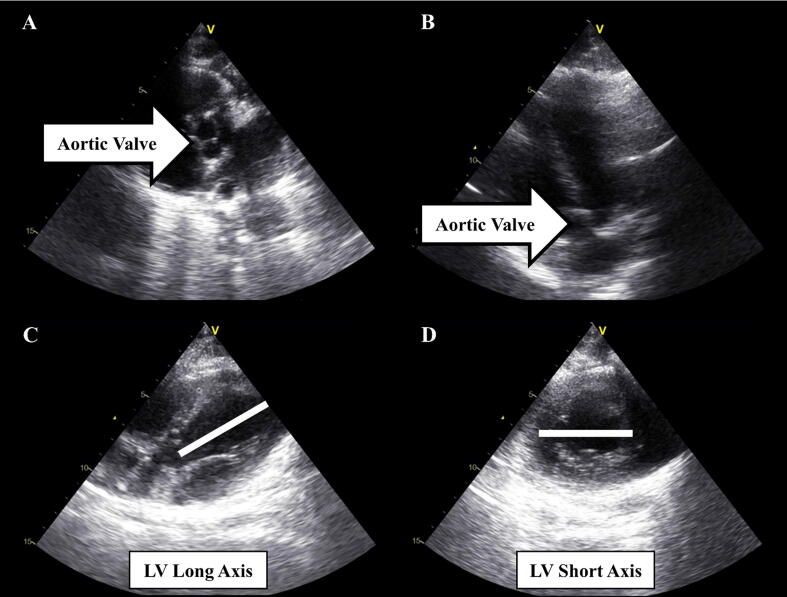
Methods: Female Landrace swine (N = 32; 35 ± 2 kg) underwent two mins of untreated asphyxiated cardiac arrest (CA). Thereafter, swine were treated with three 2-min cycles of either SCC or LVCC mechanical basic life support CPR (LUCAS 3). ETCO2 (in-line sampling), BP (arterial catheter line), and CBV (transcranial Doppler) were measured during the pre-CA, untreated-CA, and CPR-treated phases.
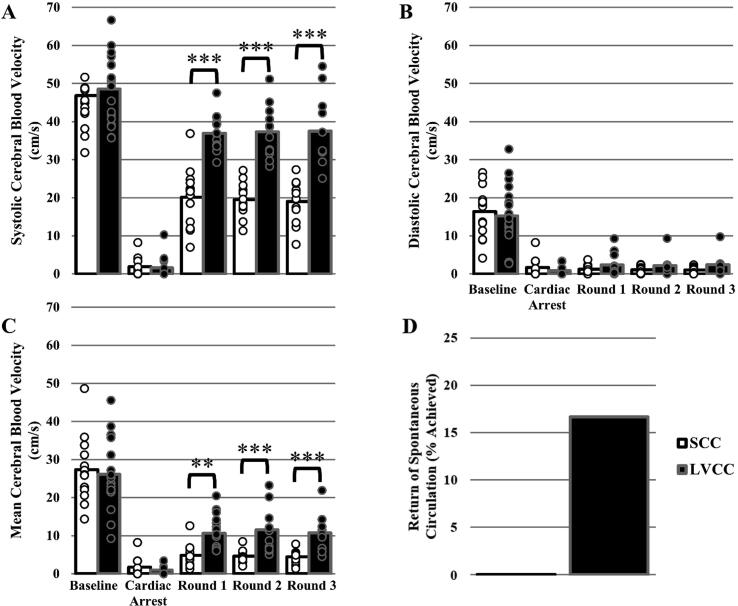
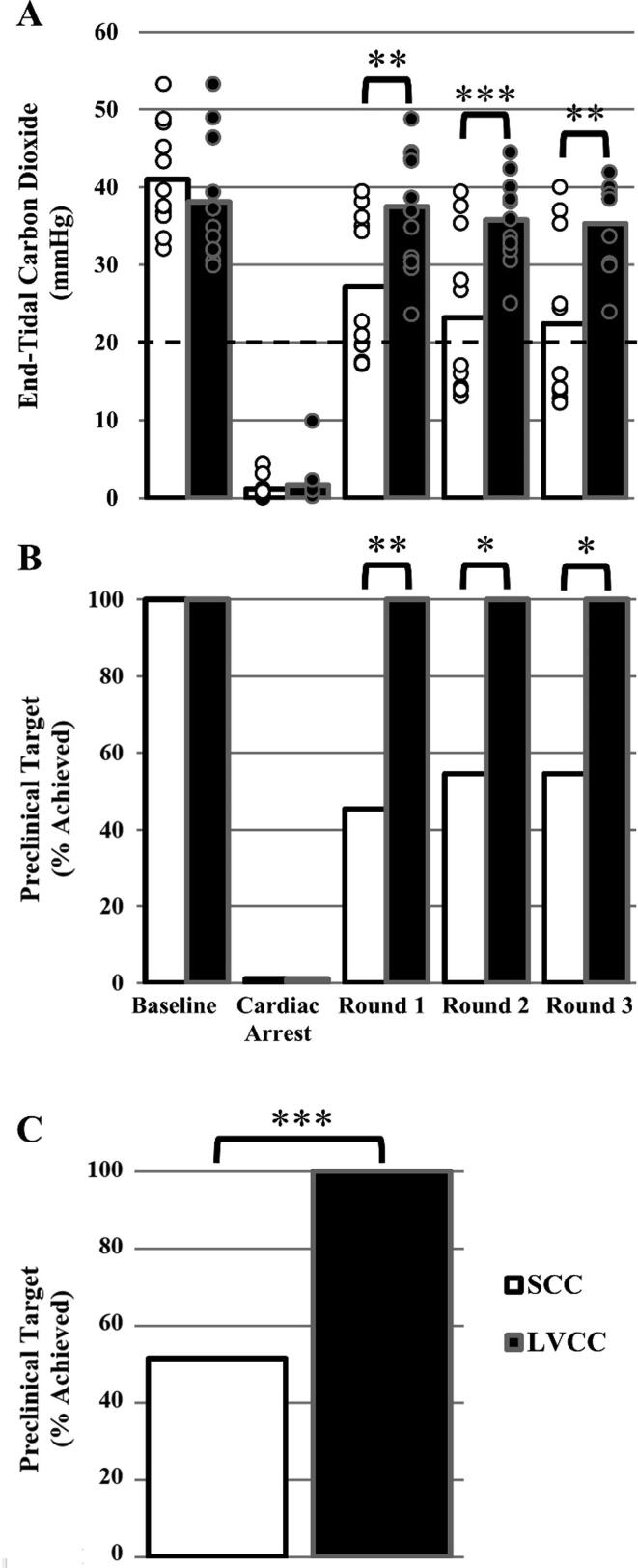
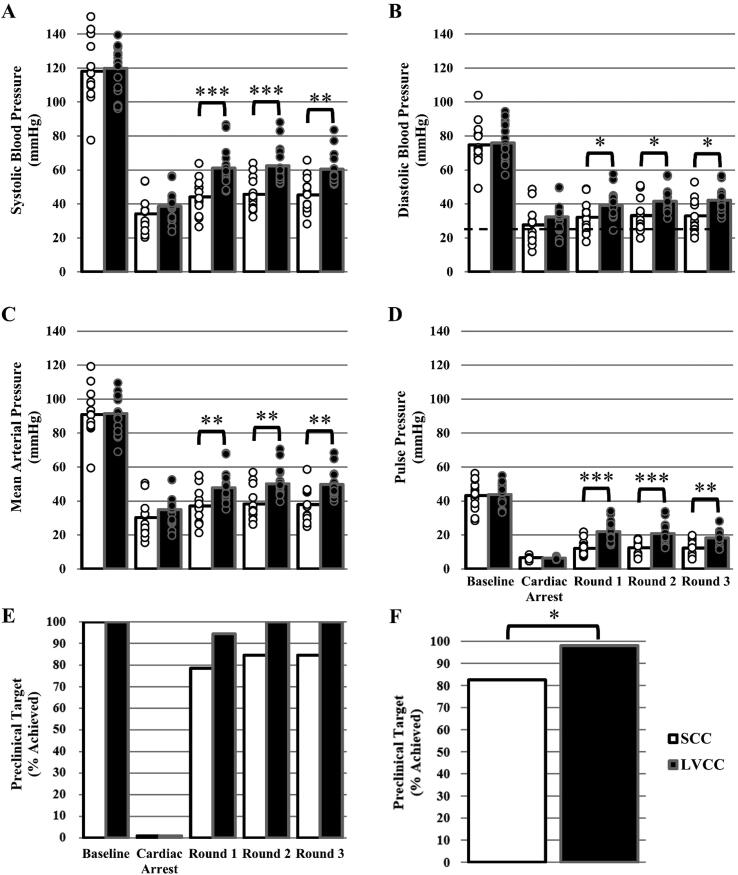
Results: ETCO2, BP, and CBV were similar between groups at pre- and during untreated-CA (P ≥ 0.188). During CPR, ETCO2 (36 ± 6 versus 24 ± 10 mmHg, P < 0.001), mean arterial BP (MAP; 49 ± 9 versus 37 ± 9 mmHg, P = 0.002), and CBV (11 ± 5 versus 5 ± 2 cm/s, P < 0.001) were significantly greater in the LVCC versus SCC group. Moreover, a greater proportion of animals obtained targets for ETCO2 (ETCO2 ≥ 20 mmHg; 52 % (17/33) versus 100 % (32/32), P < 0.001) and diastolic BP (DBP ≥ 25 mmHg; 82 % (33/40) versus 97 % (48/49), P = 0.020) in the LVCC versus SCC group.
Conclusion: Indicators of cardiac output, BP, and cerebral perfusion during CPR were greatest in the LVCC group, suggesting the quality of chest compressions during BLS CPR may be improved by performing compressions over the left ventricle compared to the centre of the chest.
Keywords: Basic Life Support; CPR; Cardiac Arrest; Cerebral Blood Flow; Chest Compressions; Left Ventricle Chest Compressions.
© 2022 The Author(s).
Figures
References
-
- Meaney P.A., Bobrow B.J., Mancini M.E., et al. Cardiopulmonary resuscitation quality: Improving cardiac resuscitation outcomes both inside and outside the hospital: A consensus statement from the American heart association. Circulation. 2013;128:417–435. doi: 10.1161/CIR.0b013e31829d8654. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
