

Machine learning nonresponse adjustment of patient-reported opioid consumption data to enable consumption-informed postoperative opioid prescribing guidelines
- PMID: 36407783
- PMCID: PMC9675048
- DOI: 10.1016/j.sipas.2022.100098
Machine learning nonresponse adjustment of patient-reported opioid consumption data to enable consumption-informed postoperative opioid prescribing guidelines
Abstract
Background: Post-discharge opioid consumption is a crucial patient-reported outcome informing opioid prescribing guidelines, but its collection is resource-intensive and vulnerable to inaccuracy due to nonresponse bias.
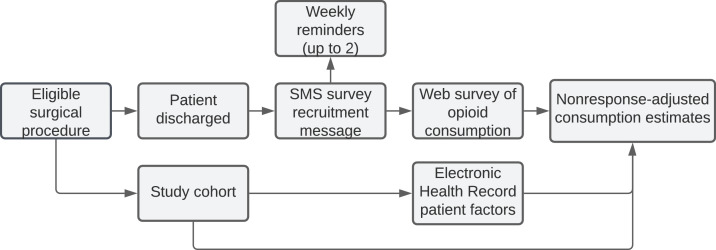
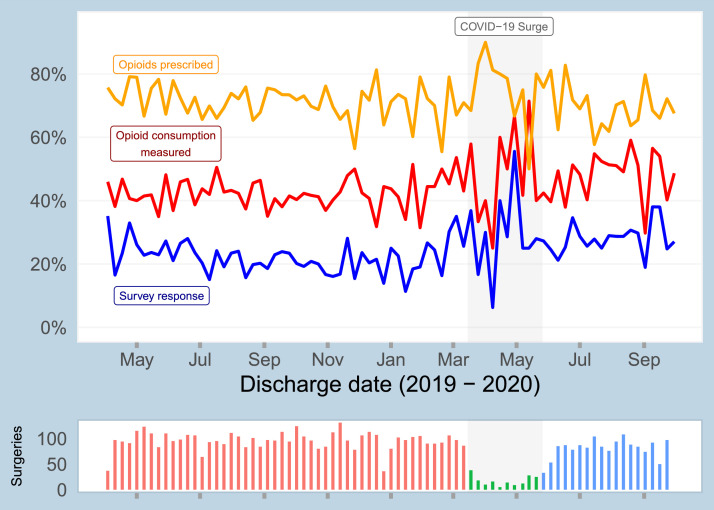
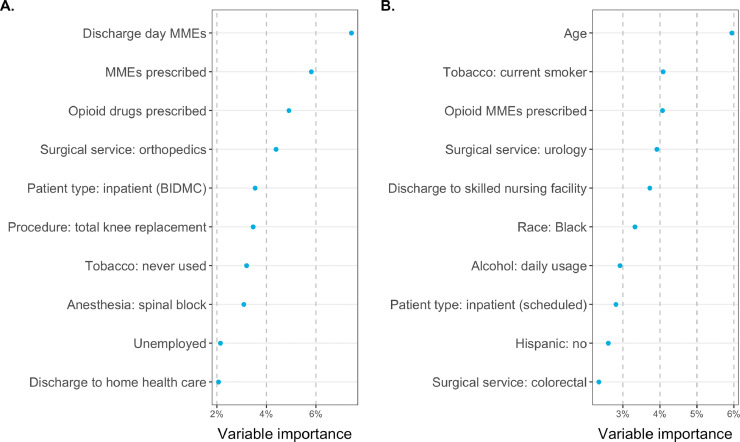
Methods: We developed a post-discharge text message-to-web survey system for efficient collection of patient-reported pain outcomes. We prospectively recruited surgical patients at Beth Israel Deaconess Medical Center in Boston, Massachusetts from March 2019 through October 2020, sending an SMS link to a secure web survey to quantify opioids consumed after discharge from hospitalization. Patient factors extracted from the electronic health record were tested for nonresponse bias and observable confounding. Following targeted learning-based nonresponse adjustment, procedure-specific opioid consumption quantiles (medians and 75th percentiles) were estimated and compared to a previous telephone-based reference survey.
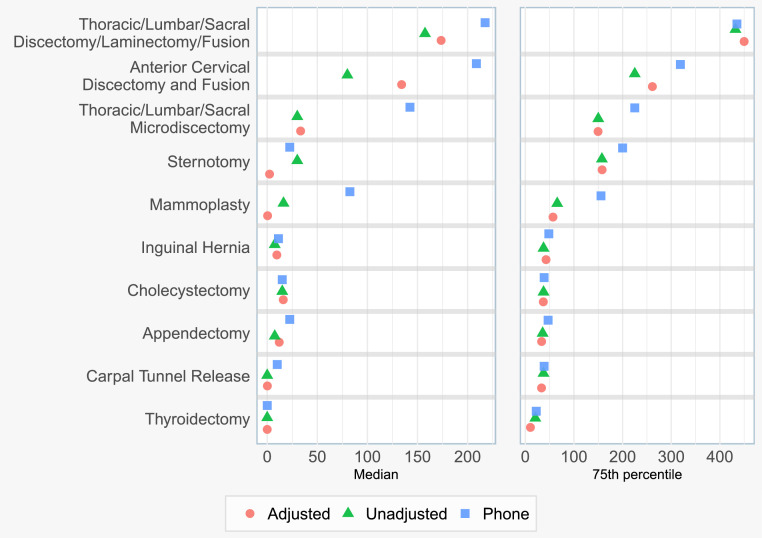
Results: 6553 patients were included. Opioid consumption was measured in 44% of patients (2868), including 21% (1342) through survey response. Characteristics associated with inability to measure opioid consumption included age, tobacco use, and prescribed opioid dose. Among the 10 most common procedures, median consumption was only 36% of the median prescription size; 64% of prescribed opioids were not consumed. Among those procedures, nonresponse adjustment corrected the median opioid consumption by an average of 37% (IQR: 7, 65%) compared to unadjusted estimates, and corrected the 75th percentile by an average of 5% (IQR: 0, 12%). This brought median estimates for 5/10 procedures closer to telephone survey-based consumption estimates, and 75th percentile estimates for 2/10 procedures closer to telephone survey-based estimates.
Conclusions: SMS-recruited online surveying can generate reliable opioid consumption estimates after nonresponse adjustment using patient factors recorded in the electronic health record, protecting patients from the risk of inaccurate prescription guidelines.
Conflict of interest statement
Declaration of Competing Interest All authors declare no competing interests.
Figures
References
-
- Hill M.V., Stucke R.S., McMahon M.L., Beeman J.L., Barth R.J. An educational intervention decreases opioid prescribing after general surgical operations. Ann Surg. 2018;267(3):468–472. - PubMed
-
- Linder B.J., Occhino J.A., Wiest S.R., Klingele C.J., Trabuco E.C., Gebhart J.B. Assessing the impact of procedure-specific opioid prescribing recommendations on opioid stewardship following pelvic organ prolapse surgery. Am J Obstet Gynecol. 2019;221(5) 515.e1-e515.e8. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
