

Investigation on the effectiveness of ventilation dilution on mitigating COVID-19 patients' secondary airway damage due to exposure to disinfectants
- PMID: 36407877
- PMCID: PMC9652096
- DOI: 10.1016/j.buildenv.2022.109787
Investigation on the effectiveness of ventilation dilution on mitigating COVID-19 patients' secondary airway damage due to exposure to disinfectants
Abstract
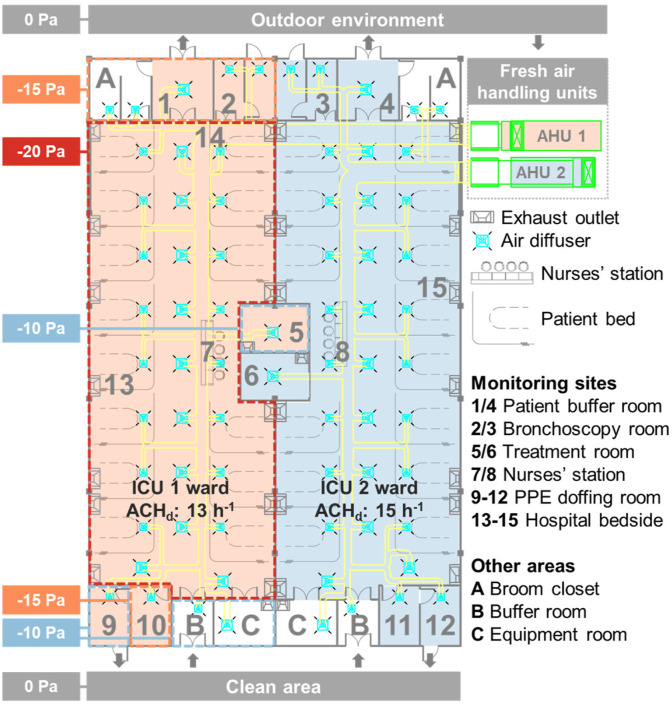
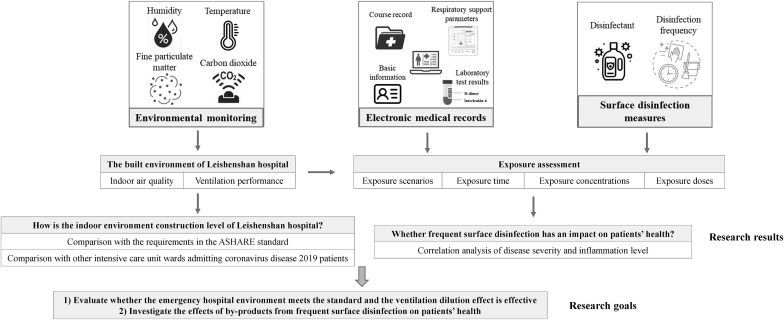
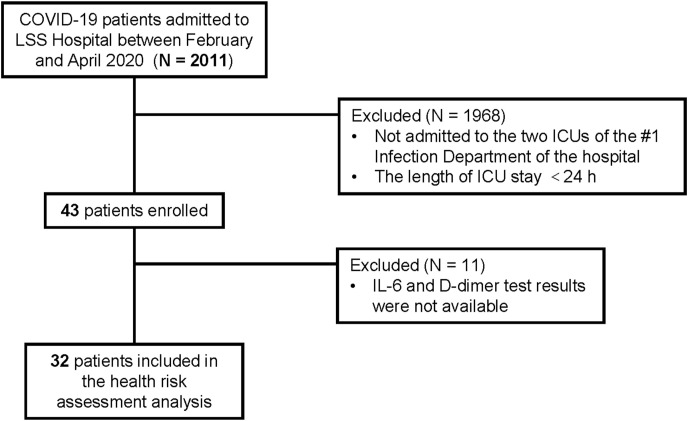
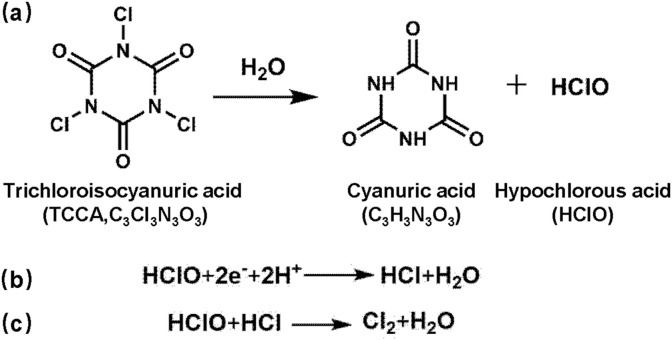
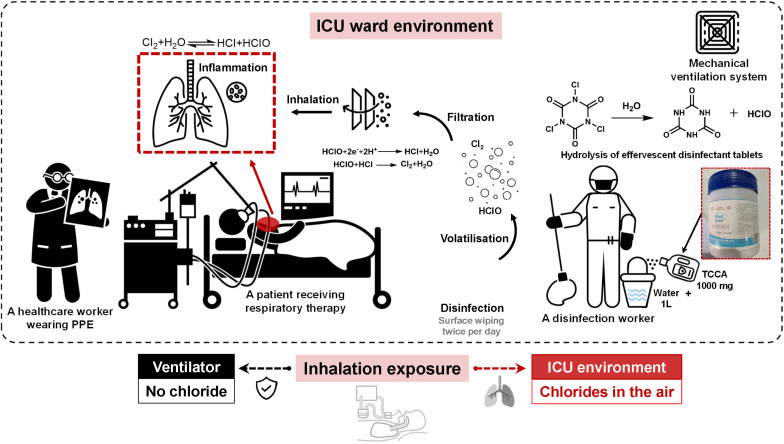
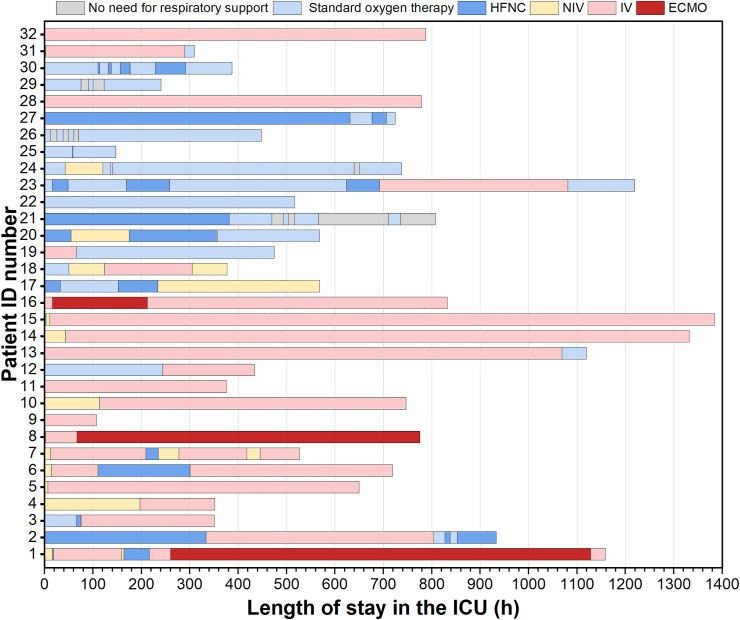
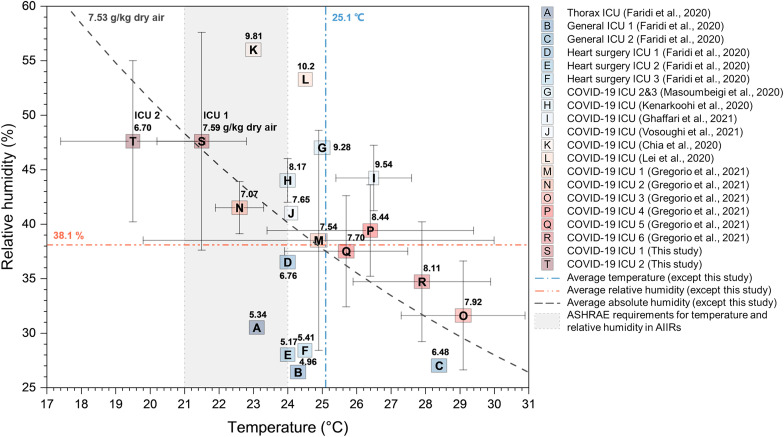
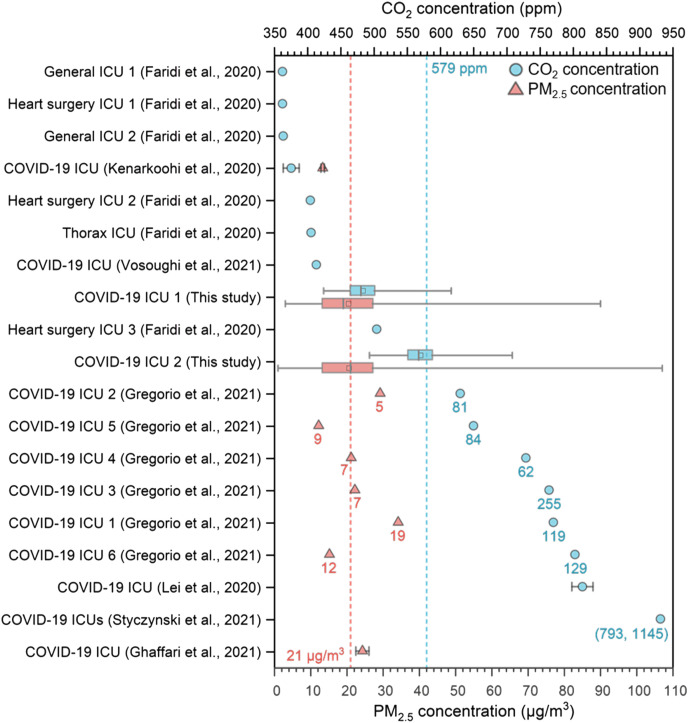
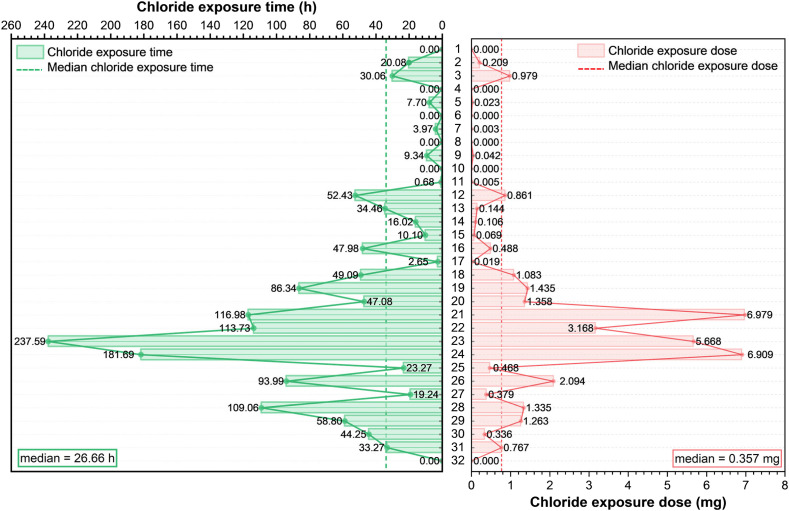
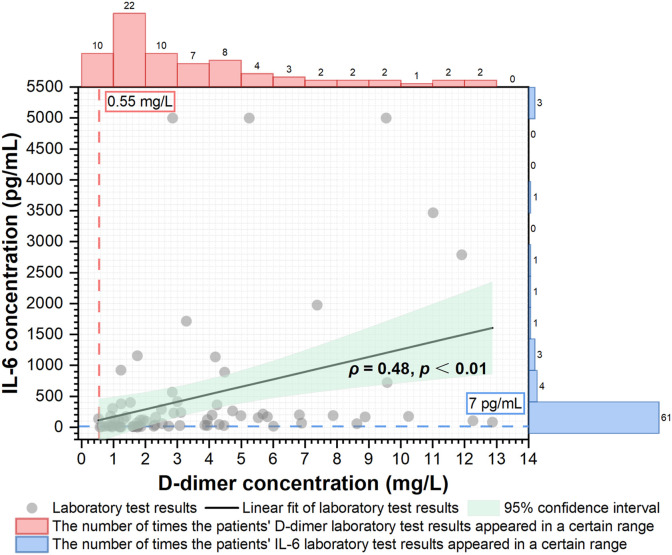
Chlorine-containing disinfectants are widely used in hospitals to prevent hospital-acquired severe acute respiratory syndrome coronavirus 2 infection. Meanwhile, ventilation is a simple but effective means to maintain clean air. It is essential to explore the exposure level and health effects of coronavirus disease 2019 patients' inhalation exposure to by-products of chloride-containing disinfectants under frequent surface disinfection and understand the role of ventilation in mitigating subsequent airway damage. We determined ventilation dilution performance and indoor air quality of two intensive care unit wards of the largest temporary hospital constructed in China, Leishenshan Hospital. The chloride inhalation exposure levels, and health risks indicated by interleukin-6 and D-dimer test results of 32 patients were analysed. The mean ± standard deviation values of the outdoor air change rate in the two intensive care unit wards were 8.8 ± 1.5 h-1 (Intensive care unit 1) and 4.1 ± 1.4 h-1 (Intensive care unit 2). The median carbon dioxide and fine particulate matter concentrations were 480 ppm and 19 μg/m3 for intensive care unit 1, and 567 ppm and 21 μg/m3 for intensive care unit 2, all of which were around the average levels of those in permanent hospitals (579 ppm and 21 μg/m3). Of these patients, the median (lower quartile, upper quartile) chloride exposure time and calculated dose were 26.66 (2.89, 57.21) h and 0.357 (0.008, 1.317) mg, respectively. A statistically significant positive correlation was observed between interleukin-6 and D-dimer concentrations. To conclude, ventilation helped maintain ward air cleanliness and health risks were not observed.
Keywords: COIVD-19; Chlorine-containing disinfectants; ICUs; Inhalation exposure.
© 2022 Published by Elsevier Ltd.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
[Standard technical specifications for methacholine chloride (Methacholine) bronchial challenge test (2023)].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Feb 12;47(2):101-119. doi: 10.3760/cma.j.cn112147-20231019-00247. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 38309959 Chinese.
-
Monitors to improve indoor air carbon dioxide concentrations in the hospital: A randomized crossover trial.Sci Total Environ. 2022 Feb 1;806(Pt 3):151349. doi: 10.1016/j.scitotenv.2021.151349. Epub 2021 Oct 30. Sci Total Environ. 2022. PMID: 34728206 Free PMC article. Clinical Trial.
-
Mortality and Morbidity Effects of Long-Term Exposure to Low-Level PM2.5, BC, NO2, and O3: An Analysis of European Cohorts in the ELAPSE Project.Res Rep Health Eff Inst. 2021 Sep;2021(208):1-127. Res Rep Health Eff Inst. 2021. PMID: 36106702 Free PMC article.
-
Environmental impacts of the widespread use of chlorine-based disinfectants during the COVID-19 pandemic.Environ Sci Pollut Res Int. 2022 Dec;29(57):85742-85760. doi: 10.1007/s11356-021-18316-2. Epub 2022 Jan 29. Environ Sci Pollut Res Int. 2022. PMID: 35091954 Free PMC article. Review.
-
Environmental and health impacts of spraying COVID-19 disinfectants with associated challenges.Environ Sci Pollut Res Int. 2022 Dec;29(57):85648-85657. doi: 10.1007/s11356-021-16575-7. Epub 2021 Oct 1. Environ Sci Pollut Res Int. 2022. PMID: 34599438 Free PMC article. Review.
References
-
- World Health Organization . 2022. WHO Coronavirus Disease (COVID-9) Dashboard.https://covid19.who.int/
-
- World Health Organization Modes of transmission of virus causing COVID-19: implications for IPC precaution recommendations. 2020. https://www.who.int/news-room/commentaries/detail/modes-of-transmission-...
LinkOut - more resources
Full Text Sources