

Contemporary use of coronary artery calcium for the allocation of aspirin in light of the 2022 USPSTF guideline recommendations
- PMID: 36407963
- PMCID: PMC9668677
- DOI: 10.1016/j.ajpc.2022.100427
Contemporary use of coronary artery calcium for the allocation of aspirin in light of the 2022 USPSTF guideline recommendations
Abstract
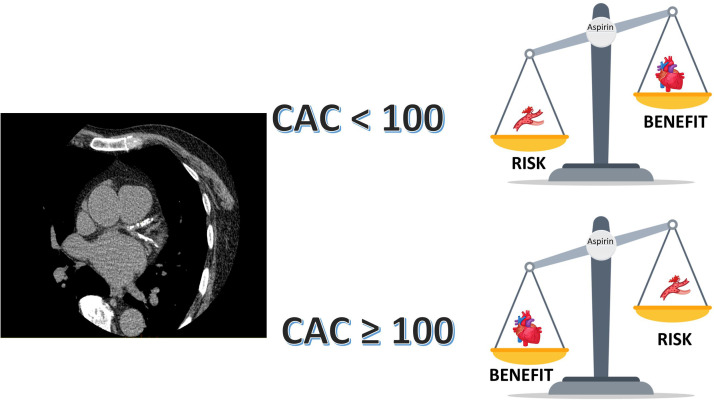
Aspirin has been a cornerstone for primary prevention of cardiovascular disease for decades, however its use in primary prevention has been challenged in recent years. The 2022 USPSTF guidelines lowered the recommendation for the use of aspirin in primary prevention based on the recent trials that demonstrated a low to neutral benefit and an increased bleeding risk with the use of aspirin in primary prevention. However, these trials enrolled patients at a relatively low risk for atherosclerotic cardiovascular disease (ASCVD) and higher bleeding risk which could have contributed to the negative results of the trials. ASCVD prevention is ideal when therapies are personalized based on individual risk. Coronary artery calcium (CAC) score is a robust marker of atherosclerosis and reliably predicts the ASCVD risk in a graded fashion. Several studies have demonstrated the use of a CAC≥100 to identify patients who will benefit from the use of aspirin in primary prevention. Furthermore, a CAC=0 identifies patients in whom aspirin would lead to net harm. In the continuum of risk from primary to secondary prevention, CAC is likely to identify the level of risk that warrants aspirin use in patients with subclinical ASCVD. The ACC/AHA 2019 primary prevention guidelines recommend the use of CAC to reclassify risk and guide personalized allocation of statins and aspirin. Although the USPSTF has not endorsed the use of CAC in the past, given an extensive body of evidence for use of CAC to guide primary preventive therapies including aspirin, it seems reasonable to use CAC to identify the level of plaque burden at which the benefit of aspirin outweighs its risk in clinical practice and personalize theallocation of aspirin in primary prevention. Future studies and randomized trials assessing the role of preventive therapies should use CAC score for risk stratification.
Keywords: ASCVD, atherosclerotic cardiovascular disease; Aspirin; Atherosclerotic cardiovascular disease; CAC, coronary artery calcium; CCTA; CCTA, Cardiac computed tomography angiography; CVD, cardiovascular disease; Coronary artery calcium; Coronary artery disease; GI, gastrointestinal; MACE, major adverse cardiovascular events; MESA, multiethnic study of atherosclerosis; MI, myocardial infarction; NNH, number needed to harm; NNT, number needed to treat; PCE, pooled cohort equation; Primary prevention; TIA, transient ischemic attack; USPSTF, united States preventive services task force.
© 2022 The Authors. Published by Elsevier B.V.
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests. None of the authors have any relationships to disclose.
Figures
References
-
- Gaziano J.M., Brotons C., Coppolecchia R., Cricelli C., Darius H., Gorelick P.B., et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a randomised, double-blind, placebo-controlled trial. Lancet. 2018;392(10152):1036–1046. - PMC - PubMed
-
- Bosetti C., Santucci C., Gallus S., Martinetti M., La Vecchia C. Aspirin and the risk of colorectal and other digestive tract cancers: an updated meta-analysis through 2019. Ann Oncol. 2020;31(5):558–568. - PubMed
-
- Bowman L., Mafham M., Wallendszus K., Stevens W., Buck G., Barton J., et al. Effects of aspirin for primary prevention in persons with diabetes mellitus. N Engl J Med. 2018;379(16):1529–1539. - PubMed
-
- Mora S., Manson J.E. Aspirin for primary prevention of atherosclerotic cardiovascular disease: advances in diagnosis and treatment. JAMA Intern Med. 2016;176(8):1195–1204. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
