

Analysis of postoperative effects of different semicircular canal surgical technique in patients with labyrinthine fistulas
- PMID: 36408412
- PMCID: PMC9669453
- DOI: 10.3389/fnins.2022.1032087
Analysis of postoperative effects of different semicircular canal surgical technique in patients with labyrinthine fistulas
Abstract
Objective: Different semicircular canal surgery techniques have been used to treat patients with labyrinthine fistulas caused by middle ear cholesteatoma. This study evaluated postoperative hearing and vestibular function after various semicircular canal surgeries.
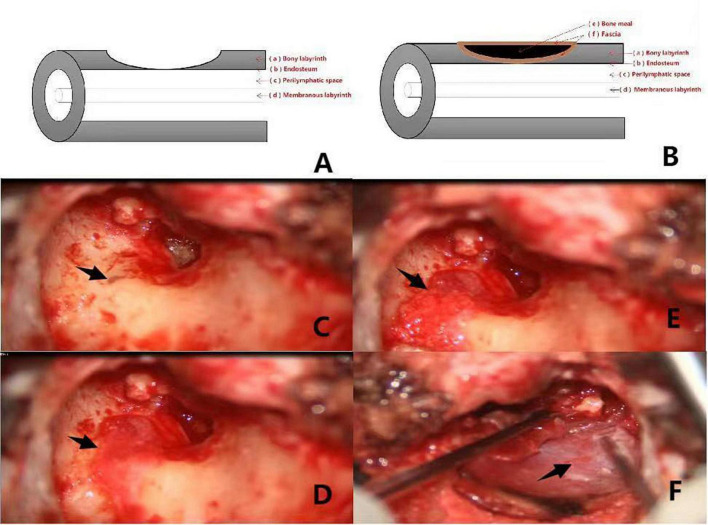
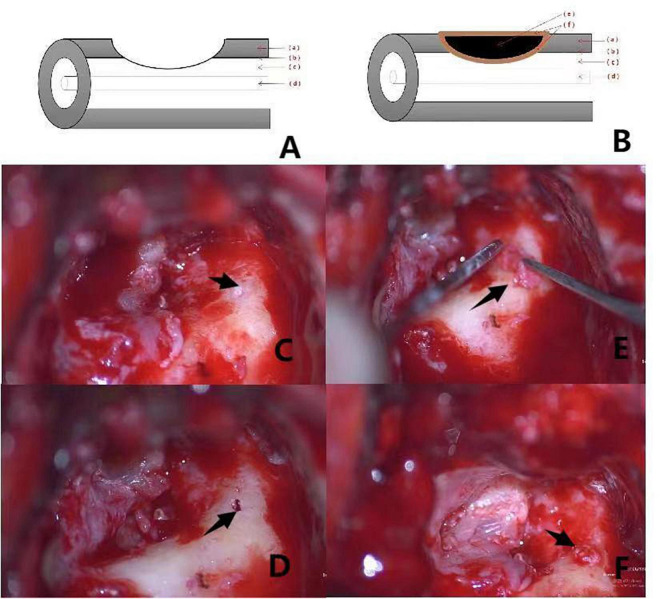
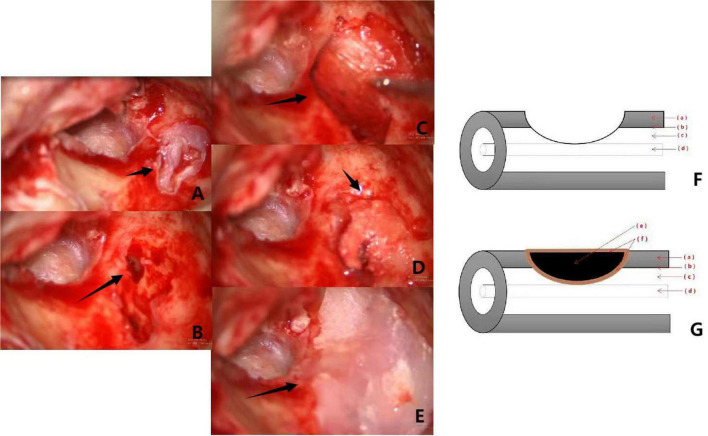
Materials and methods: In group 1, from January 2008 to December 2014, 29 patients with middle ear cholesteatoma complicated by labyrinthine fistulas were treated with surgery involving covering the fistulas with simple fascia. In group 2, from January 2015 to October 2021, 36 patients with middle ear cholesteatoma complicated by labyrinthine fistulas were included. Cholesteatomas on the surface of type I labyrinthine fistulas were cleaned using the "under water technique" and capped with a "sandwich" composed of fascia, bone meal, and fascia. Cholesteatomas on the surface of type II and III fistulas were cleaned using the "under water technique," and the labyrinthine fistula was plugged with a "pie" composed of fascia, bone meal, and fascia, and then covered with bone wax.
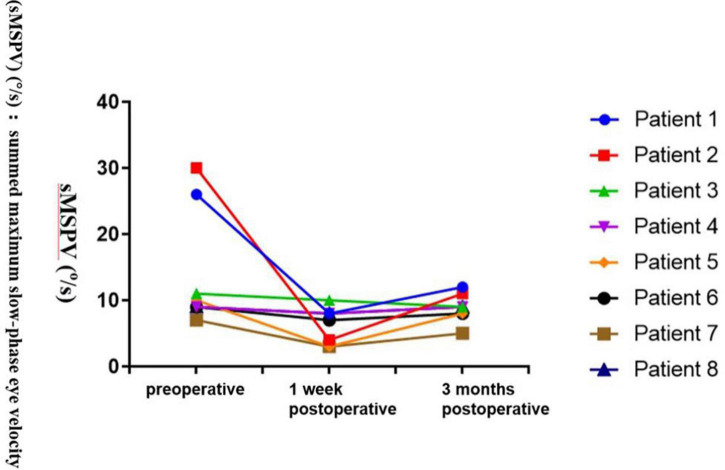
Results: Some patients with labyrinthine fistulas in group 1 exhibited symptoms of vertigo after surgery. In group 2 Patients with type II labyrinthine fistulas experienced short-term vertigo after semicircular canal occlusion, but no cases of vertigo were reported during long-term follow-up. "sandwich." In patients with type II labyrinthine fistulas, the semicircular canal occlusion influenced postoperative hearing improvement. However, postoperative patient hearing was still superior to preoperative hearing.
Conclusion: The surface of type I labyrinthine fistulas should be capped by a "sandwich" composed of fascia, bone meal, and fascia. Type II and III labyrinthine fistulas should be plugged with a "pie" composed of fascia, bone meal, and fascia, covered with bone wax.
Keywords: analysis; hearing; labyrinthine fistula; middle ear cholesteatoma; semicircular canal occlusion.
Copyright © 2022 Meng, Cai, Gao, Ji, Sun, Li, Wei, Chen, Ni, Yan and He.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Lateral semicircular canal fistula in cholesteatoma: diagnosis and management.Eur Arch Otorhinolaryngol. 2016 Aug;273(8):2055-63. doi: 10.1007/s00405-015-3775-6. Epub 2015 Sep 8. Eur Arch Otorhinolaryngol. 2016. PMID: 26351038
-
Clinical efficacy of the 'sandwich technique' in repairing cholesteatoma with labyrinthine fistula.Acta Otolaryngol. 2022 Jan;142(1):30-35. doi: 10.1080/00016489.2021.2022207. Epub 2022 Jan 8. Acta Otolaryngol. 2022. PMID: 35001839
-
Labyrinthine Fistula-Our Experience at a Tertiary Hospital.Indian J Otolaryngol Head Neck Surg. 2022 Aug;74(Suppl 1):88-92. doi: 10.1007/s12070-020-01857-2. Epub 2020 Apr 17. Indian J Otolaryngol Head Neck Surg. 2022. PMID: 36032823 Free PMC article.
-
[Studies of labyrinthine cholesteatoma-related fistulas: report of 22 cases].J Otolaryngol. 2005 Feb;34(1):1-6. doi: 10.2310/7070.2005.00001. J Otolaryngol. 2005. PMID: 15966468 Review. French.
-
Development of semicircular canal occlusion.Front Neurosci. 2022 Aug 19;16:977323. doi: 10.3389/fnins.2022.977323. eCollection 2022. Front Neurosci. 2022. PMID: 36061608 Free PMC article.
Cited by
-
Identification of miRNA expression profile in middle ear cholesteatoma using small RNA-sequencing.BMC Med Genomics. 2024 Jun 18;17(1):162. doi: 10.1186/s12920-024-01932-5. BMC Med Genomics. 2024. PMID: 38890701 Free PMC article.
-
[Semicircular canal occlusion].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2024 Feb;38(2):122-126. doi: 10.13201/j.issn.2096-7993.2024.02.008. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2024. PMID: 38297865 Free PMC article. Review. Chinese.
References
LinkOut - more resources
Full Text Sources