

Sex and age differences in the Multiple Sclerosis prodrome
- PMID: 36408518
- PMCID: PMC9668896
- DOI: 10.3389/fneur.2022.1017492
Sex and age differences in the Multiple Sclerosis prodrome
Abstract
Background and objectives: Little is known of the potential sex and age differences in the MS prodrome. We investigated sex and age differences in healthcare utilization during the MS prodrome.
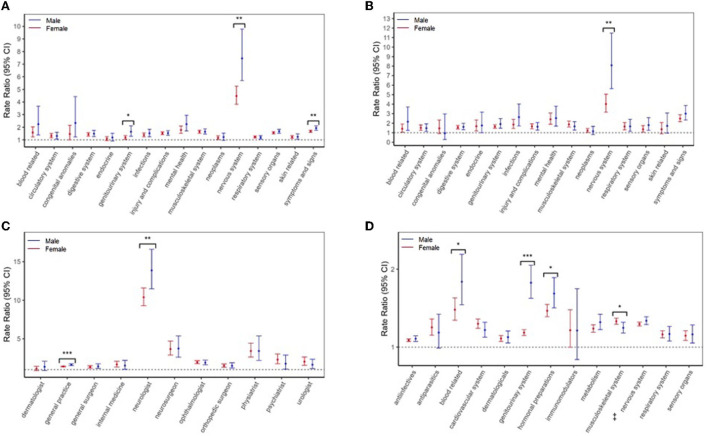
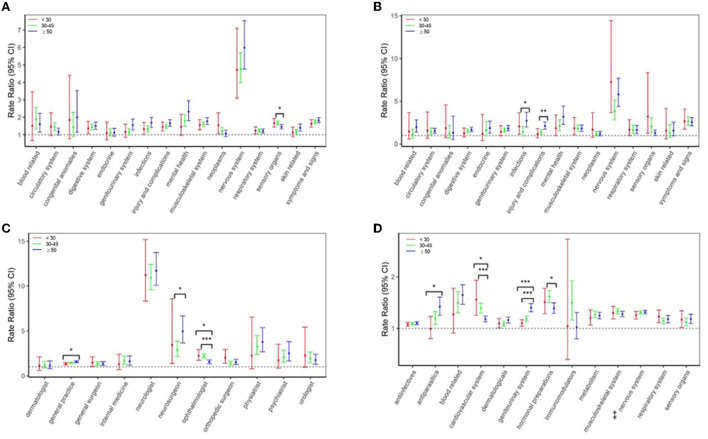
Methods: This was a population-based matched cohort study linking administrative and clinical data from British Columbia, Canada (population = 5 million). MS cases in the 5 years preceding a first demyelinating event ("administrative cohort;" n = 6,863) or MS symptom onset ("clinical cohort;" n = 966) were compared to age-, sex- and geographically-matched controls (n = 31,865/4,534). Negative binomial and modified Poisson models were used to compare the rates of physician visits and hospitalizations per international classification of diseases chapter, and prescriptions filled per drug class, between MS cases and controls across sex and age-groups (< 30, 30-49, ≥50 years).
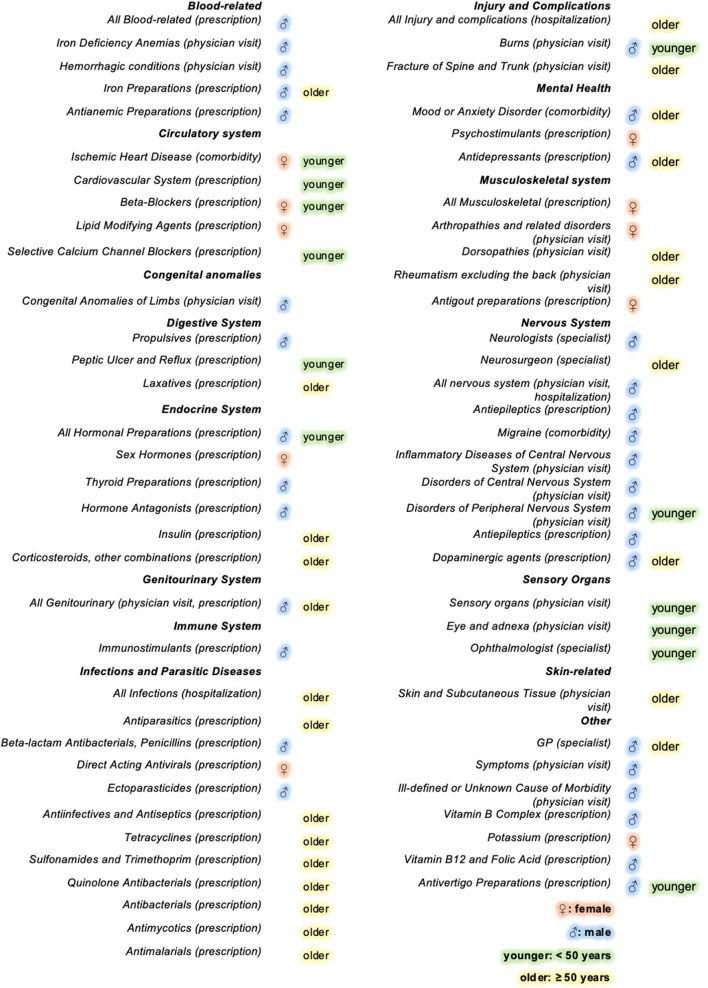
Results: In the administrative cohort, males with MS had a higher relative rate for genitourinary-related visits (males: adjusted Rate Ratio (aRR) = 1.65, females: aRR = 1.19, likelihood ratio test P = 0.02) and antivertigo prescriptions (males: aRR = 4.72, females: aRR = 3.01 P < 0.01). Injury and infection-related hospitalizations were relatively more frequent for ≥50-year-olds (injuries < 30/30-49/≥50: aRR = 1.16/1.39/2.12, P < 0.01; infections 30-49/≥50: aRR = 1.43/2.72, P = 0.03), while sensory-related visits and cardiovascular prescriptions were relatively more common in younger persons (sensory 30-49/≥50: aRR = 1.67/1.45, P = 0.03; cardiovascular < 30/30-49/≥50: aRR = 1.56/1.39/1.18, P < 0.01). General practitioner visits were relatively more frequent in males (males: aRR = 1.63, females: aRR = 1.40, P < 0.01) and ≥50-year-olds (< 30/≥50: aRR = 1.32/1.55, P = 0.02), while differences in ophthalmologist visits were disproportionally larger among younger persons, < 50-years-old (< 30/30-49/≥50: aRR = 2.25/2.20/1.55, P < 0.01). None of the sex and age-related differences in the smaller clinical cohort reached significance (P ≥ 0.05).
Discussion: Sex and age-specific differences in healthcare use were observed in the 5 years before MS onset. Findings demonstrate fundamental heterogeneity in the MS prodromal presentation.
Keywords: Multiple Sclerosis; age; healthcare use; prodromal; sex.
Copyright © 2022 Yusuf, Wijnands, Karim, Kingwell, Zhu, Evans, Fisk, Zhao, Marrie and Tremlett.
Conflict of interest statement
Author FY was funded by a Fredrick Banting and Charles Best Canada Graduate Scholarship from the Canadian Institutes of Health Research (CIHR). Author JF receives research funding from: CIHR, Crohn's and Colitis Canada, Research Nova Scotia; consultation and distribution royalties from MAPI Research Trust. Over the past 4 years, Author MK has received consulting fees from Biogen (unrelated to the current project) and participated in Advisory Boards and/or Satellite Symposia of Biogen Inc. Author RM receives research funding from: CIHR, Research Manitoba, Multiple Sclerosis Society of Canada, Multiple Sclerosis Scientific Foundation, Crohn's and Colitis Canada, National Multiple Sclerosis Society, CMSC. She was supported by the Waugh Family Chair in Multiple Sclerosis. She was a co-investigator on studies funded partly by Biogen Idec and Roche (no funds to her, her institution). Author HT has, in the last 5 years, received research support from the Canada Research Chair Program, the National Multiple Sclerosis Society, the Canadian Institutes of Health Research, the Multiple Sclerosis Society of Canada and the Multiple Sclerosis Scientific Research Foundation. In addition, in the last 5 years, has had travel expenses or registration fees prepaid or reimbursed to present at CME conferences from the Consortium of MS Centres (2018), National MS Society (2016, 2018), ECTRIMS/ACTRIMS (2015, 2016, 2017, 2018, 2019, 2020, 2021, 2022), American Academy of Neurology (2015, 2016, 2019). Speaker honoraria are either declined or donated to an MS charity or to an unrestricted grant for use by HT's research group. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Gastrointestinal conditions in the multiple sclerosis prodrome.Ann Clin Transl Neurol. 2024 Jan;11(1):185-193. doi: 10.1002/acn3.51945. Epub 2023 Dec 19. Ann Clin Transl Neurol. 2024. PMID: 38115680 Free PMC article.
-
Psychiatric Comorbidity During the Prodromal Period in Patients With Multiple Sclerosis.Neurology. 2023 Nov 14;101(20):e2026-e2034. doi: 10.1212/WNL.0000000000207843. Epub 2023 Sep 25. Neurology. 2023. PMID: 37748884 Free PMC article.
-
Infection-related health care utilization among people with and without multiple sclerosis.Mult Scler. 2017 Oct;23(11):1506-1516. doi: 10.1177/1352458516681198. Epub 2016 Dec 21. Mult Scler. 2017. PMID: 28273769
-
Predictors of Loss to Follow-Up in an HIV Vaccine Preparedness Study in Masaka, Uganda.Int J Environ Res Public Health. 2022 May 24;19(11):6377. doi: 10.3390/ijerph19116377. Int J Environ Res Public Health. 2022. PMID: 35681962 Free PMC article. Review.
-
The multiple sclerosis prodrome.Nat Rev Neurol. 2021 Aug;17(8):515-521. doi: 10.1038/s41582-021-00519-3. Epub 2021 Jun 21. Nat Rev Neurol. 2021. PMID: 34155379 Free PMC article. Review.
Cited by
-
Prodromal multiple sclerosis: considerations and future utility.J Neurol. 2024 Apr;271(4):2129-2140. doi: 10.1007/s00415-023-12173-4. Epub 2024 Feb 11. J Neurol. 2024. PMID: 38341810 Free PMC article. Review.
-
Reduced childbirth rates in multiple sclerosis from the prodromal phase: Evidence from a population-based cohort study.Mult Scler. 2025 Apr;31(4):398-407. doi: 10.1177/13524585251315077. Epub 2025 Feb 17. Mult Scler. 2025. PMID: 39957514 Free PMC article.
-
Phenotyping Healthcare Use 2-3 Decades Before the First Multiple Sclerosis Demyelinating Event.Ann Clin Transl Neurol. 2025 Aug;12(8):1585-1594. doi: 10.1002/acn3.70092. Epub 2025 Jun 12. Ann Clin Transl Neurol. 2025. PMID: 40503873 Free PMC article.
-
Association Between Diseases and Symptoms Diagnosed in Primary Care and the Subsequent Specific Risk of Multiple Sclerosis.Neurology. 2023 Dec 12;101(24):e2497-e2508. doi: 10.1212/WNL.0000000000207981. Epub 2023 Nov 29. Neurology. 2023. PMID: 38052493 Free PMC article.
-
Health Care Use Before Multiple Sclerosis Symptom Onset.JAMA Netw Open. 2025 Aug 1;8(8):e2524635. doi: 10.1001/jamanetworkopen.2025.24635. JAMA Netw Open. 2025. PMID: 40748636 Free PMC article.
References
LinkOut - more resources
Full Text Sources