

Revascularization improves vascular hemodynamics - a study assessing cerebrovascular reserve and transit time in Moyamoya patients using MRI
- PMID: 36408536
- PMCID: PMC10638998
- DOI: 10.1177/0271678X221140343
Revascularization improves vascular hemodynamics - a study assessing cerebrovascular reserve and transit time in Moyamoya patients using MRI
Abstract
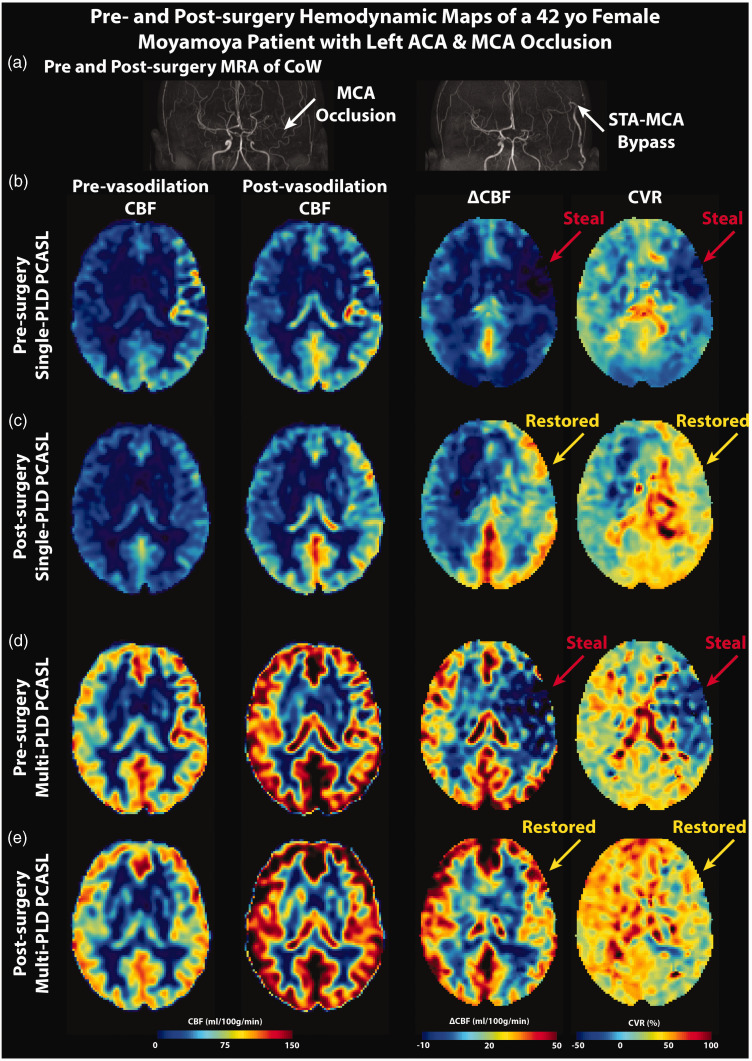
Cerebrovascular reserve (CVR) reflects the capacity of cerebral blood flow (CBF) to change. Decreased CVR implies poor hemodynamics and is linked to a higher risk for stroke. Revascularization has been shown to improve CBF in patients with vasculopathy such as Moyamoya disease. Dynamic susceptibility contrast (DSC) can measure transit time to evaluate patients suspected of stroke. Arterial spin labeling (ASL) is a non-invasive technique for CBF, CVR, and arterial transit time (ATT) measurements. Here, we investigate the change in hemodynamics 4-12 months after extracranial-to-intracranial direct bypass in 52 Moyamoya patients using ASL with single and multiple post-labeling delays (PLD). Images were collected using ASL and DSC with acetazolamide. CVR, CBF, ATT, and time-to-maximum (Tmax) were measured in different flow territories. Results showed that hemodynamics improved significantly in regions affected by arterial occlusions after revascularization. CVR increased by 16 ± 11% (p < 0.01) and 25 ± 13% (p < 0.01) for single- and multi-PLD ASL, respectively. Transit time measured by multi-PLD ASL and post-vasodilation DSC reduced by 13 ± 7% (p < 0.01) and 9 ± 5% (p < 0.01), respectively. For all regions, ATT correlated significantly with Tmax (R2 = 0.59, p < 0.01). Thus, revascularization improved CVR and decreased transit times. Multi-PLD ASL can serve as an effective and non-invasive modality to examine vascular hemodynamics in Moyamoya patients.
Keywords: Arterial spin labeling; Moyamoya disease; arterial transit time; cerebral blood flow; cerebrovascular reserve.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Greg Zaharchuk received funding support through GE Healthcare and Bayer Healthcare and equity from Subtle Medical. Gary Steinberg is a consultant for SanBio, Zeiss, and Surgical Theater, and receives royalties from Peter Lazic, US. The conflicts of interest were all unrelated to the current study.
Figures





Similar articles
-
Short- and Long-Term MRI Assessed Hemodynamic Changes in Pediatric Moyamoya Patients After Revascularization.J Magn Reson Imaging. 2024 Apr;59(4):1349-1357. doi: 10.1002/jmri.28902. Epub 2023 Jul 29. J Magn Reson Imaging. 2024. PMID: 37515518
-
Using arterial spin labeling to measure cerebrovascular reactivity in Moyamoya disease: Insights from simultaneous PET/MRI.J Cereb Blood Flow Metab. 2022 Aug;42(8):1493-1506. doi: 10.1177/0271678X221083471. Epub 2022 Mar 2. J Cereb Blood Flow Metab. 2022. PMID: 35236136 Free PMC article.
-
Cerebrovascular reactivity measurements using simultaneous 15O-water PET and ASL MRI: Impacts of arterial transit time, labeling efficiency, and hematocrit.Neuroimage. 2021 Jun;233:117955. doi: 10.1016/j.neuroimage.2021.117955. Epub 2021 Mar 11. Neuroimage. 2021. PMID: 33716155 Free PMC article.
-
Clinical utility of arterial spin labeling imaging in disorders of the nervous system.Neurosurg Focus. 2019 Dec 1;47(6):E5. doi: 10.3171/2019.9.FOCUS19567. Neurosurg Focus. 2019. PMID: 31786550 Review.
-
Quantitative hemodynamic studies in moyamoya disease: a review.Neurosurg Focus. 2009 Apr;26(4):E5. doi: 10.3171/2009.1.FOCUS08300. Neurosurg Focus. 2009. PMID: 19335131 Free PMC article. Review.
Cited by
-
Three-dimensional pseudocontinuous arterial spin labeling with dual postlabeling delay for reflecting cerebral blood flow regulation in patients with hydrocephalus: a retrospective cross-sectional study.Quant Imaging Med Surg. 2024 Aug 1;14(8):5861-5876. doi: 10.21037/qims-24-151. Epub 2024 Jul 30. Quant Imaging Med Surg. 2024. PMID: 39143996 Free PMC article.
-
Characterizing pre- and post-operative cerebral blood flow and transit time in pediatric moyamoya patients using multi-delay ASL and DSC MRI.J Cereb Blood Flow Metab. 2025 Jul 15:271678X251358979. doi: 10.1177/0271678X251358979. Online ahead of print. J Cereb Blood Flow Metab. 2025. PMID: 40665679 Free PMC article.
-
Effects of antiplatelet therapy on reducing stroke risk in patients with moyamoya disease: the role of postcontrast MR vessel wall imaging.Eur Radiol. 2025 Apr 11. doi: 10.1007/s00330-025-11562-9. Online ahead of print. Eur Radiol. 2025. PMID: 40214736
-
Recommendations for quantitative cerebral perfusion MRI using multi-timepoint arterial spin labeling: Acquisition, quantification, and clinical applications.Magn Reson Med. 2024 Aug;92(2):469-495. doi: 10.1002/mrm.30091. Epub 2024 Apr 9. Magn Reson Med. 2024. PMID: 38594906 Free PMC article. Review.
-
Recent advances in mechanistic, therapeutic, and diagnostic research of cerebrovascular diseases: updates from brain & BrainPET 2022.J Cereb Blood Flow Metab. 2023 Nov;43(2_suppl):4-7. doi: 10.1177/0271678X231183290. Epub 2023 Aug 17. J Cereb Blood Flow Metab. 2023. PMID: 37589500 Free PMC article.
References
-
- Kassner A, Winter JD, Poublanc J, et al.. Blood-oxygen level dependent MRI measures of cerebrovascular reactivity using a controlled respiratory challenge: reproducibility and gender differences. J Magn Reson Imaging JMRI 2010; 31: 298–304. - PubMed
-
- Endo H, Inoue T, Ogasawara K, et al.. Quantitative assessment of cerebral hemodynamics using perfusion-weighted MRI in patients with major cerebral artery occlusive disease: comparison with positron emission tomography. Stroke J Cereb Circ 2006; 37: 388–392. - PubMed
-
- Totaro R, Marini C, Baldassarre M, et al.. Cerebrovascular reactivity evaluated by transcranial doppler: Reproducibility of different methods. Cerebrovasc Dis 1999; 9: 142–145. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
