

Serum insulin-like growth factor binding protein 3 as a promising diagnostic and prognostic biomarker in esophagogastric junction adenocarcinoma
- PMID: 36409444
- PMCID: PMC9679126
- DOI: 10.1007/s12672-022-00591-1
Serum insulin-like growth factor binding protein 3 as a promising diagnostic and prognostic biomarker in esophagogastric junction adenocarcinoma
Abstract
Background: Esophagogastric junction adenocarcinoma (EJA) lacks serum biomarkers to assist in diagnosis and prognosis. Here, we aimed to evaluate the diagnostic and prognostic value of serum insulin-like growth factor binding protein 3 (IGFBP3) in EJA patients.
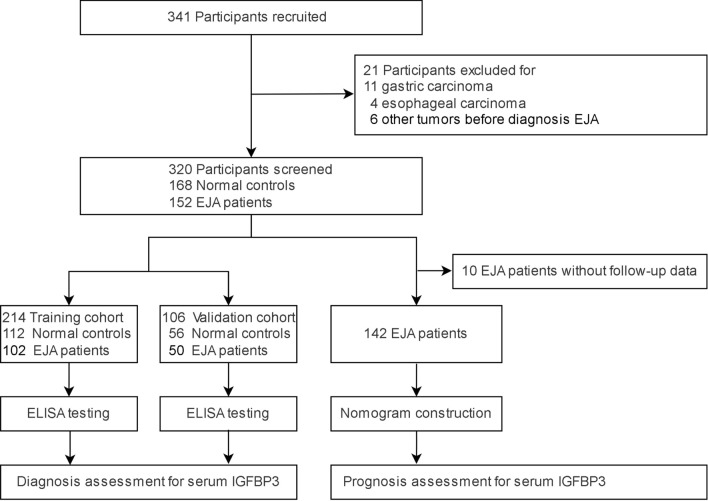
Methods: 320 participants were recruited from November 2016 to January 2020, who were randomly divided into a training cohort (112 normal controls and 102 EJA patients including 24 early-stage patients) and a validation cohort (56 normal controls and 50 EJA patients including 12 early-stage patients). We used receiver operating characteristics curve (ROC) to evaluate diagnostic value. The predictive performance of the nomogram was evaluated by the concordance index (C-index).
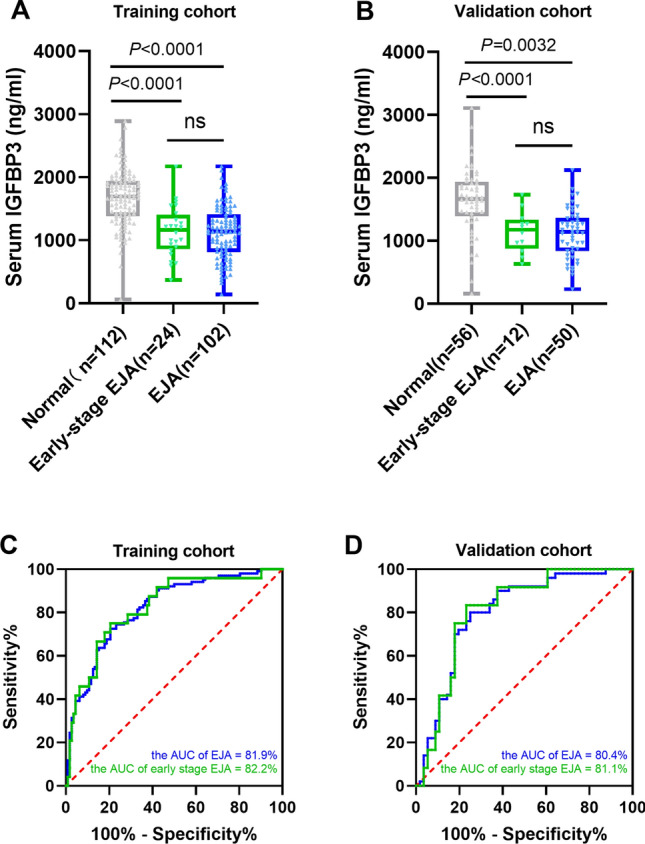
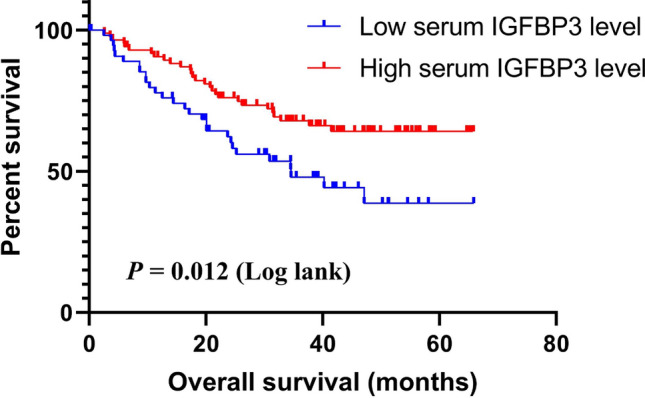
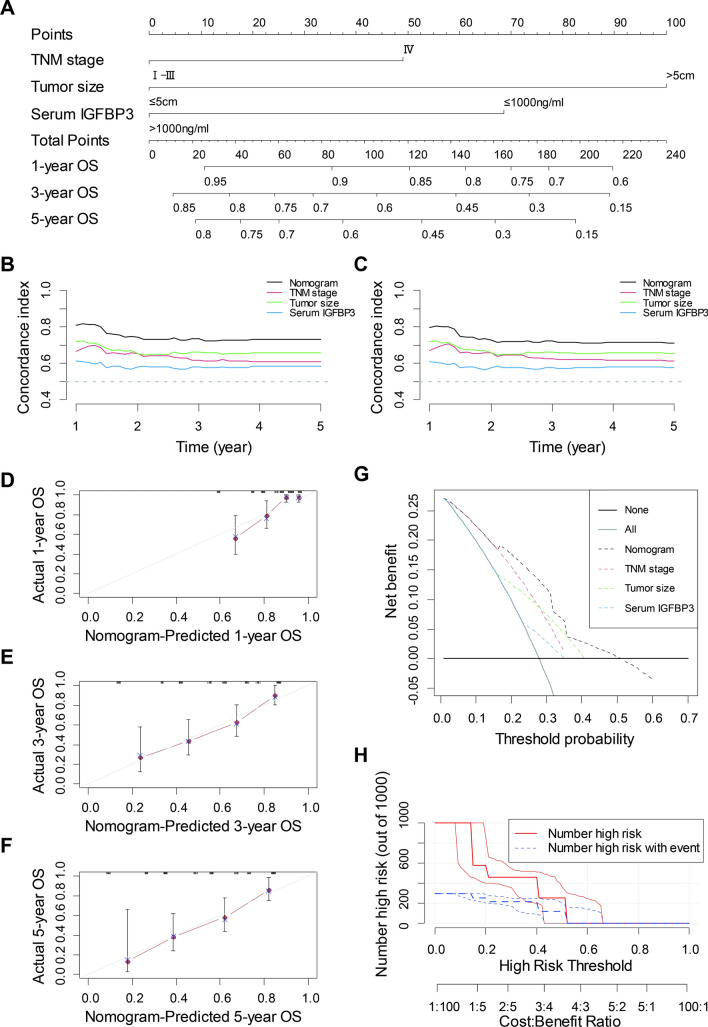
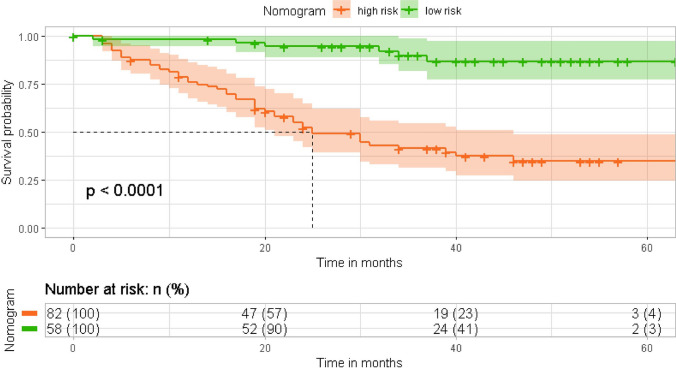
Results: Serum IGFBP3 levels were significantly lower in early-stage EJA or EJA patients than those in controls (P < 0.01). Measurement of serum IGFBP3 demonstrated an area under curve of 0.819, specificity 90.18% and sensitivity 43.14% in training cohort. Similar results were observed in validation cohort (0.804, 87.50%, 42.00%). Importantly, serum IGFBP3 had a satisfactory diagnostic value for early-stage EJA (0.822, 90.18%, 45.83% and 0.811, 84.48%, 50.00% in training and validation cohorts, respectively). Furthermore, survival analysis demonstrated that lower serum IGFBP3 level was related to poor prognosis (P < 0.05). Cox multivariate analysis revealed that serum IGFBP3 was an independent prognostic factor (HR = 0.468, P = 0.005). Compared with TNM stage, a nomogram based on serum IGFBP3, tumor size and TNM stage indicated an improved C-index in prognostic prediction (0.625 vs. 0.735, P = 0.001).
Conclusions: We found that serum IGFBP3 was a potential diagnostic and prognostic marker of EJA. Meanwhile, the nomogram might predict the prognosis of EJA more accurately and efficiently.
Keywords: Diagnosis; Esophagogastric junction adenocarcinoma; IGFBP3; Nomogram; Prognosis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Serum insulin-like growth factor binding protein-3 as a potential biomarker for diagnosis and prognosis of oesophageal squamous cell carcinoma.Ann Med. 2022 Dec;54(1):2153-2166. doi: 10.1080/07853890.2022.2104921. Ann Med. 2022. PMID: 35930383 Free PMC article.
-
Serum Insulin-Like Growth Factor Binding Protein 7 as a Potential Biomarker in the Diagnosis and Prognosis of Esophagogastric Junction Adenocarcinoma.Gut Liver. 2020 Nov 15;14(6):727-734. doi: 10.5009/gnl19135. Gut Liver. 2020. PMID: 31822054 Free PMC article.
-
Combined detection of serum autoantibodies as diagnostic biomarkers in esophagogastric junction adenocarcinoma.Gastric Cancer. 2019 May;22(3):546-557. doi: 10.1007/s10120-018-0894-y. Epub 2018 Nov 13. Gastric Cancer. 2019. PMID: 30426295 Free PMC article.
-
Serum DSG2 as a potential biomarker for diagnosis of esophageal squamous cell carcinoma and esophagogastric junction adenocarcinoma.Biosci Rep. 2022 May 27;42(5):BSR20212612. doi: 10.1042/BSR20212612. Biosci Rep. 2022. PMID: 35521959 Free PMC article.
-
Blood-based Markers in the Prognostic Prediction of Esophagogastric Junction Cancer.J Cancer. 2020 Apr 27;11(15):4332-4342. doi: 10.7150/jca.44545. eCollection 2020. J Cancer. 2020. PMID: 32489452 Free PMC article. Review.
Cited by
-
Nomograms for prognosis prediction in esophageal adenocarcinoma: realities and challenges.Clin Transl Oncol. 2025 Feb;27(2):449-457. doi: 10.1007/s12094-024-03589-z. Epub 2024 Jul 31. Clin Transl Oncol. 2025. PMID: 39083141 Review.
-
BNIPL is a promising biomarker of laryngeal cancer: novel insights from bioinformatics analysis and experimental validation.BMC Med Genomics. 2024 Feb 1;17(1):45. doi: 10.1186/s12920-024-01811-z. BMC Med Genomics. 2024. PMID: 38302910 Free PMC article.
-
Multiomics combined with single-cell analysis shows that mitophagy-related genes could accurately predict the prognosis of patients with clear cell renal cell carcinoma.Transl Cancer Res. 2024 Feb 29;13(2):819-832. doi: 10.21037/tcr-23-1765. Epub 2024 Feb 23. Transl Cancer Res. 2024. PMID: 38482447 Free PMC article.
-
Diabetes Mellitus and Gastric Cancer: Correlation and Potential Mechanisms.J Diabetes Res. 2023 Nov 9;2023:4388437. doi: 10.1155/2023/4388437. eCollection 2023. J Diabetes Res. 2023. PMID: 38020199 Free PMC article. Review.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous