

Noninferiority of Posterior Cervical Foraminotomy vs Anterior Cervical Discectomy With Fusion for Procedural Success and Reduction in Arm Pain Among Patients With Cervical Radiculopathy at 1 Year: The FACET Randomized Clinical Trial
- PMID: 36409485
- PMCID: PMC9679957
- DOI: 10.1001/jamaneurol.2022.4208
Noninferiority of Posterior Cervical Foraminotomy vs Anterior Cervical Discectomy With Fusion for Procedural Success and Reduction in Arm Pain Among Patients With Cervical Radiculopathy at 1 Year: The FACET Randomized Clinical Trial
Abstract
Importance: The choice between posterior cervical foraminotomy (posterior surgery) and anterior cervical discectomy with fusion (anterior surgery) for cervical foraminal radiculopathy remains controversial.
Objective: To investigate the noninferiority of posterior vs anterior surgery in patients with cervical foraminal radiculopathy with regard to clinical outcomes after 1 year.
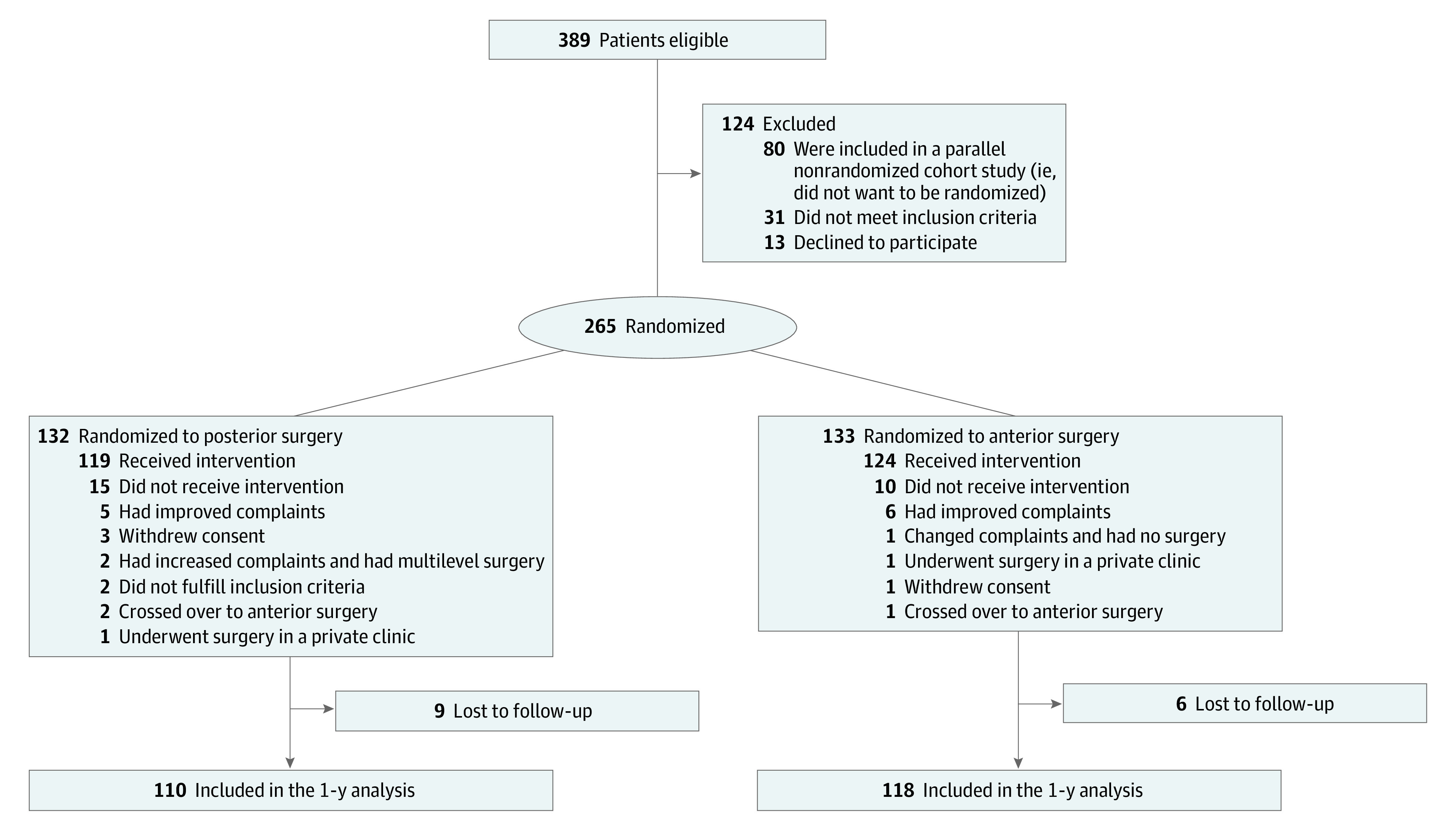
Design, setting, and participants: This multicenter investigator-blinded noninferiority randomized clinical trial was conducted from January 2016 to May 2020 with a total follow-up of 2 years. Patients were included from 9 hospitals in the Netherlands. Of 389 adult patients with 1-sided single-level cervical foraminal radiculopathy screened for eligibility, 124 declined to participate or did not meet eligibility criteria. Patients with pure axial neck pain without radicular pain were not eligible. Of 265 patients randomized (132 to posterior and 133 to anterior), 15 were lost to follow-up and 228 were included in the 1-year analysis (110 in posterior and 118 in anterior).
Interventions: Patients were randomly assigned 1:1 to posterior foraminotomy or anterior cervical discectomy with fusion.
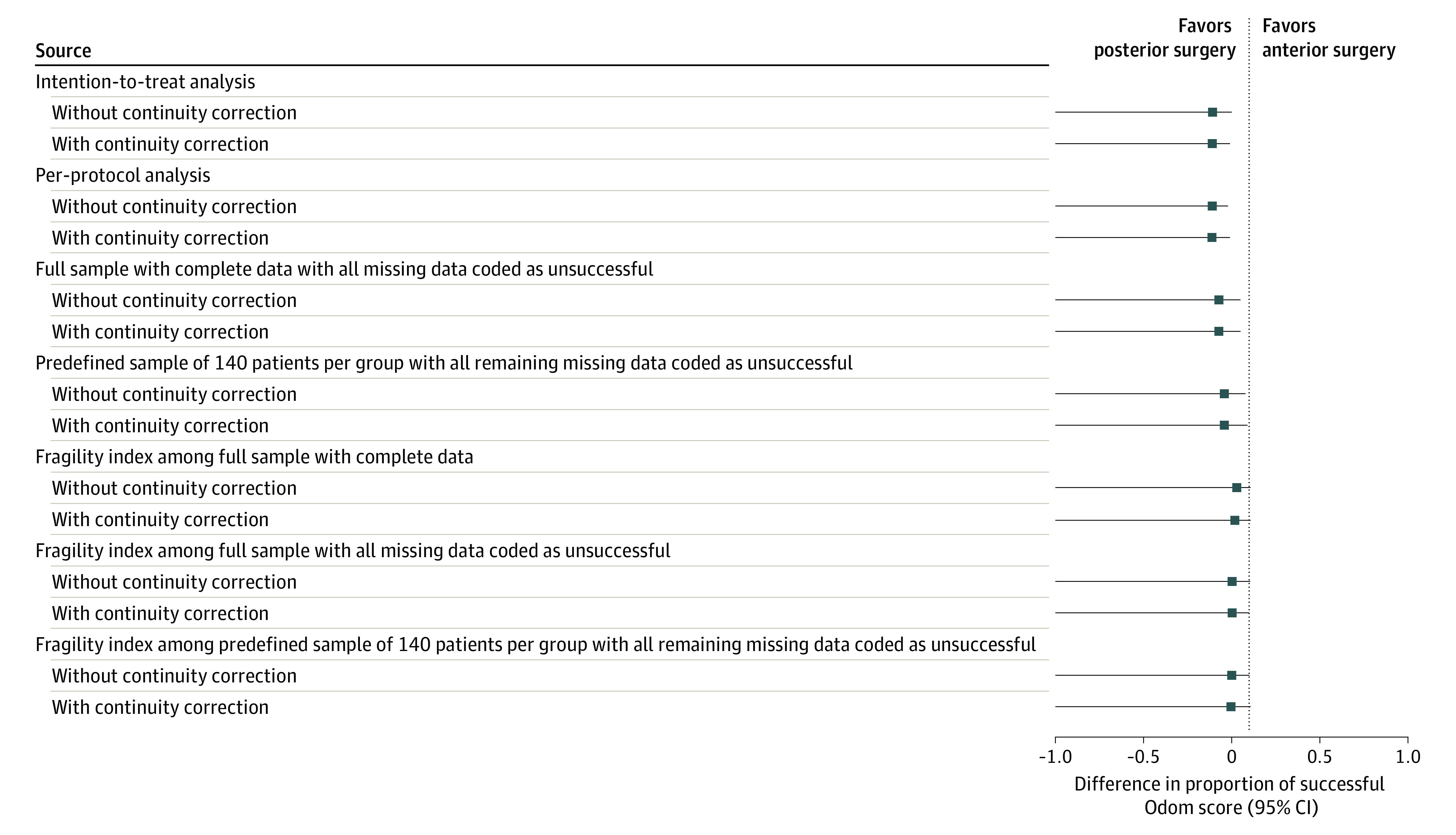
Main outcomes and measures: Primary outcomes were proportion of success using Odom criteria and decrease in arm pain using a visual analogue scale from 0 to 100 with a noninferiority margin of 10% (assuming advantages with posterior surgery over anterior surgery that would justify a tolerable loss of efficacy of 10%). Secondary outcomes were neck pain, disability, quality of life, work status, treatment satisfaction, reoperations, and complications. Analyses were performed with 2-proportion z tests at 1-sided .05 significance levels with Bonferroni corrections.
Results: Among 265 included patients, the mean (SD) age was 51.2 (8.3) years; 133 patients (50%) were female and 132 (50%) were male. Patients were randomly assigned to posterior (132) or anterior (133) surgery. The proportion of success was 0.88 (86 of 98) in the posterior surgery group and 0.76 (81 of 106) in the anterior surgery group (difference, -0.11 percentage points; 1-sided 95% CI, -0.01) and the between-group difference in arm pain was -2.8 (1-sided 95% CI, -9.4) at 1-year follow-up, indicating noninferiority of posterior surgery. Decrease in arm pain had a between-group difference of 3.4 (1-sided 95% CI, 11.8), crossing the noninferiority margin with 1.8 points. All secondary outcomes had 2-sided 95% CIs clustered around 0 with small between-group differences.
Conclusions and relevance: In this randomized clinical trial, posterior surgery was noninferior to anterior surgery for patients with cervical radiculopathy regarding success rate and arm pain at 1 year. Decrease in arm pain and secondary outcomes had small between-group differences. These results may be used to enhance shared decision-making.
Trial registration: Netherlands Trial Register Identifier: NTR5536.
Conflict of interest statement
Figures
References
-
- Broekema AEH, Groen RJM, Tegzess E, Reneman MF, Soer R, Kuijlen JMA. Anterior or posterior approach in the surgical treatment of cervical radiculopathy; neurosurgeons’ preference in the Netherlands. Interdiscip Neurosurg. 2021;23. doi: 10.1016/j.inat.2020.100930 - DOI
