

Trends and Risk Factors for Venous Thromboembolism Among Hospitalized Medical Patients
- PMID: 36409498
- PMCID: PMC9679881
- DOI: 10.1001/jamanetworkopen.2022.40373
Trends and Risk Factors for Venous Thromboembolism Among Hospitalized Medical Patients
Abstract
Importance: While hospital-associated venous thromboembolism (HA-VTE) is a known complication of hospitalization, contemporary incidence and outcomes data are scarce and methodologically contested.
Objective: To define and validate an automated electronic health record (EHR)-based algorithm for retrospective detection of HA-VTE and examine contemporary HA-VTE incidence, previously reported risk factors, and outcomes.
Design, setting, and participants: This cohort study was conducted using hospital admissions between January 1, 2013, and June 30, 2021, with follow-up until December 31, 2021. All medical (non-intensive care unit) admissions at an integrated health care delivery system with 21 hospitals in Northern California during the study period were included. Data were analyzed from January to June 2022.
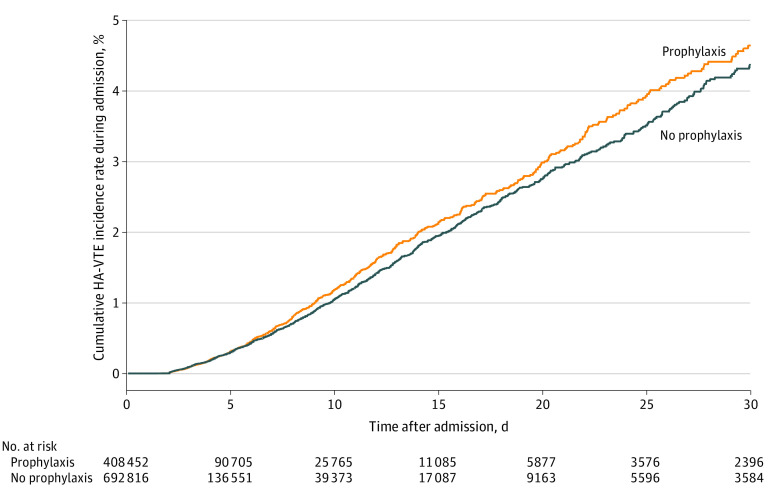
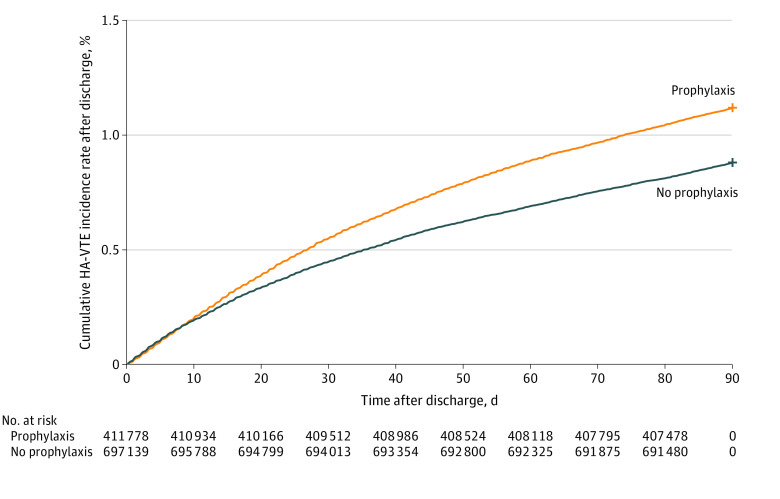
Exposures: Previously reported risk factors associated with HA-VTE and administration of pharmacological prophylaxis were evaluated as factors associated with HA-VTE.
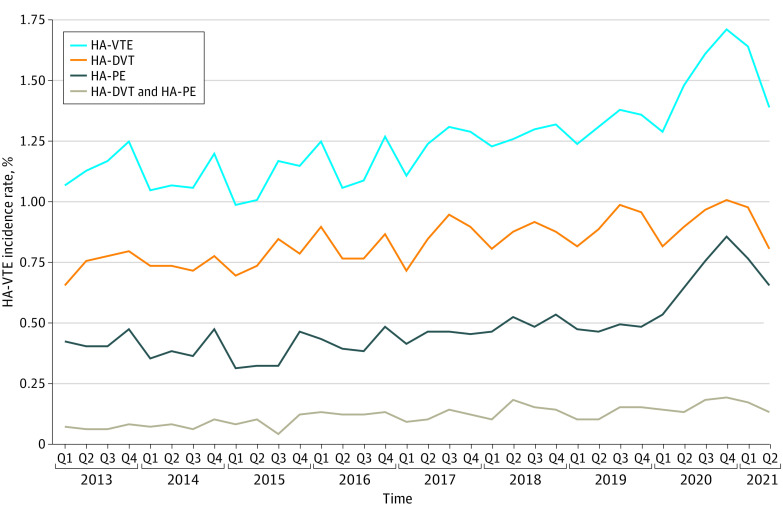
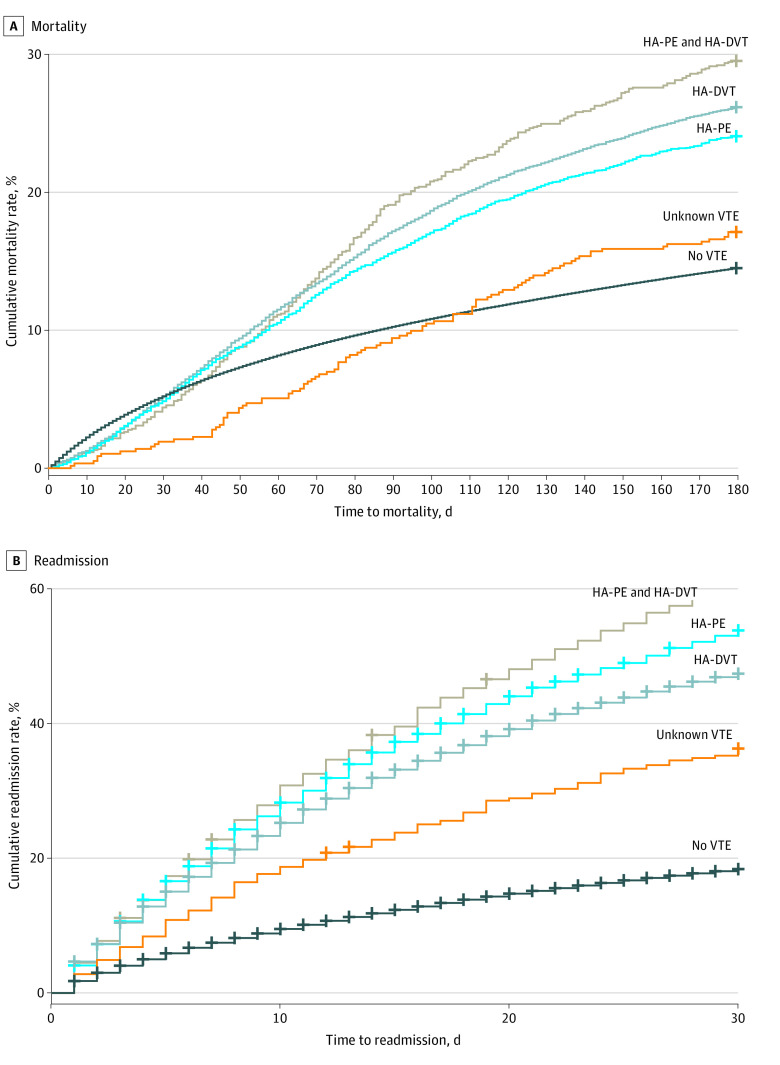
Main outcomes and measures: Yearly incidence rates and timing of HA-VTE events overall and by subtype (deep vein thrombosis, pulmonary embolism, both, or unknown), as well as readmissions and mortality rates.
Results: Among 1 112 014 hospitalizations involving 529 492 patients (268 797 [50.8%] women; 75 238 Asian [14.2%], 52 697 Black [10.0%], 79 398 Hispanic [15.0%], and 307 439 non-Hispanic White [58.1%]; median [IQR] age, 67.0 [54.0-79.0] years), there were 13 843 HA-VTE events (1.2% of admissions) occurring in 10 410 patients (2.0%). HA-VTE events increased from 307 of 29 095 hospitalizations (1.1%) in the first quarter of 2013 to 551 of 33 729 hospitalizations (1.6%) in the first quarter of 2021. Among all HA-VTE events, 10 746 events (77.6%) were first noted after discharge. In multivariable analyses, several factors were associated with increased odds of HA-VTE, including active cancer (adjusted odds ratio [aOR], 1.96; 95% CI, 1.85-2.08), prior VTE (aOR, 1.71; 95% CI, 1.63-1.79), and reduced mobility (aOR, 1.63; 95% CI, 1.50-1.77). Factors associated with decreased likelihood of HA-VTE included Asian race (vs non-Hispanic White: aOR, 0.65; 95% CI, 0.61-0.69), current admission for suspected stroke (aOR, 0.73; 95% CI, 0.65-0.81), and Hispanic ethnicity (vs non-Hispanic White: aOR, 0.81; 95% CI, 0.77-0.86). HA-VTE events were associated with increased risk of readmission (hazard ratio [HR], 3.33; 95% CI, 3.25-3.41) and mortality (HR, 1.63; 95% CI, 1.57-1.70).
Conclusions and relevance: This study found that HA-VTE events occurred in 1.2% of medical admissions, increased over time, and were associated with increased adverse outcomes. These findings suggest that approaches designed to mitigate occurrence and outcomes associated with HA-VTE may remain needed.
Conflict of interest statement
Figures
Similar articles
-
A Three-year Retrospective Study Looking at Preventing Hospital Acquired Thrombosis.Cardiovasc Hematol Agents Med Chem. 2024;22(2):212-222. doi: 10.2174/0118715257269027231228114930. Cardiovasc Hematol Agents Med Chem. 2024. PMID: 38288832
-
Hospital performance for pharmacologic venous thromboembolism prophylaxis and rate of venous thromboembolism : a cohort study.JAMA Intern Med. 2014 Oct;174(10):1577-84. doi: 10.1001/jamainternmed.2014.3384. JAMA Intern Med. 2014. PMID: 25133488
-
Prevalence and risk factors of hospital acquired venous thromboembolism.Phlebology. 2025 May;40(4):266-274. doi: 10.1177/02683555241297566. Epub 2024 Nov 5. Phlebology. 2025. PMID: 39499060
-
Trends in Venous Thromboembolism Anticoagulation in Patients Hospitalized With COVID-19.JAMA Netw Open. 2021 Jun 1;4(6):e2111788. doi: 10.1001/jamanetworkopen.2021.11788. JAMA Netw Open. 2021. PMID: 34115129 Free PMC article.
-
Factors associated with venous thromboembolism pharmacoprophylaxis initiation in hospitalized medical patients: the Medical Inpatients Thrombosis and Hemostasis study.J Thromb Haemost. 2024 Dec;22(12):3521-3531. doi: 10.1016/j.jtha.2024.08.016. Epub 2024 Sep 12. J Thromb Haemost. 2024. PMID: 39260742
Cited by
-
Factors Associated with Hospital Length of Stay among VTE Cases: Insights from the i-RegVed Registry.J Prim Care Community Health. 2024 Jan-Dec;15:21501319241266815. doi: 10.1177/21501319241266815. J Prim Care Community Health. 2024. PMID: 39118386 Free PMC article.
-
Who dies from venous thromboembolism after hospitalisation for other reasons in England?: a national retrospective cohort study.BMJ Open. 2024 May 20;14(5):e082951. doi: 10.1136/bmjopen-2023-082951. BMJ Open. 2024. PMID: 38772580 Free PMC article.
-
Development and validation of machine learning models for postoperative venous thromboembolism prediction in colorectal cancer inpatients: a retrospective study.J Gastrointest Oncol. 2023 Feb 28;14(1):220-232. doi: 10.21037/jgo-23-18. Epub 2023 Feb 15. J Gastrointest Oncol. 2023. PMID: 36915444 Free PMC article.
-
Development and evaluation of a national administrative code-based system for estimation of hospital-acquired venous thromboembolism in Ireland.BMJ Open. 2025 Feb 20;15(2):e084951. doi: 10.1136/bmjopen-2024-084951. BMJ Open. 2025. PMID: 39979043 Free PMC article.
-
Racial, biological sex, and geographic disparities of venous thromboembolism in the United States, 2016 to 2019.J Vasc Surg Venous Lymphat Disord. 2024 Sep;12(5):101908. doi: 10.1016/j.jvsv.2024.101908. Epub 2024 May 15. J Vasc Surg Venous Lymphat Disord. 2024. PMID: 38759751 Free PMC article.
