

Human Immunodeficiency Virus (HIV) Care Continuum Outcomes After Transition to Adult Care Among a Prospective Cohort of Youth With HIV in Atlanta, Georgia
- PMID: 36409586
- PMCID: PMC10319754
- DOI: 10.1093/cid/ciac904
Human Immunodeficiency Virus (HIV) Care Continuum Outcomes After Transition to Adult Care Among a Prospective Cohort of Youth With HIV in Atlanta, Georgia
Abstract
Background: Healthcare transition from pediatric to adult-oriented clinical settings is often viewed as a high-risk time for care disengagement. However, there is a paucity of prospective, longitudinal research documenting human immunodeficiency virus (HIV) care outcomes after healthcare transition.
Methods: We conducted a prospective, observational cohort study of healthcare transition among youth enrolled at an HIV care center in Atlanta, Georgia. Pediatric clinic patients (average age, 24 years) were enrolled up to 3 months before the expected transition and were followed up to determine linkage, retention, and viral suppression in adult care through electronic medical record abstractions at the baseline and at 6, 12, 18, and 24 months.
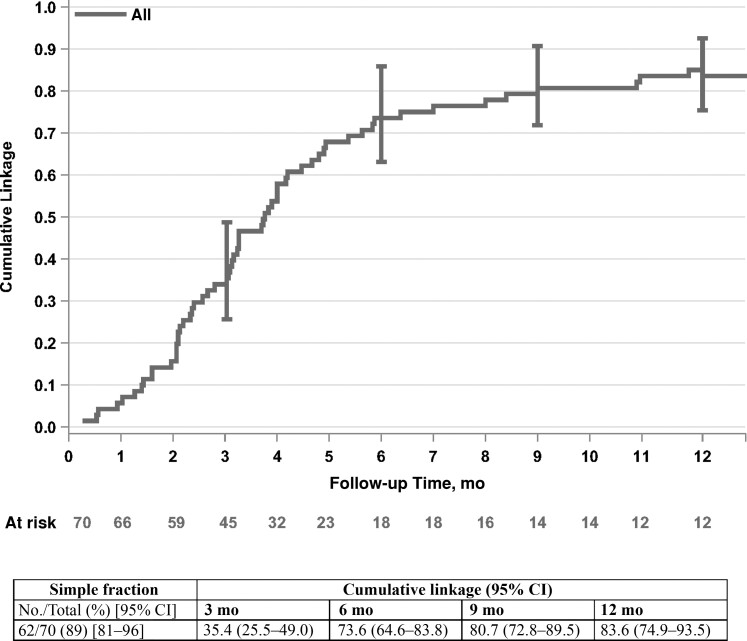
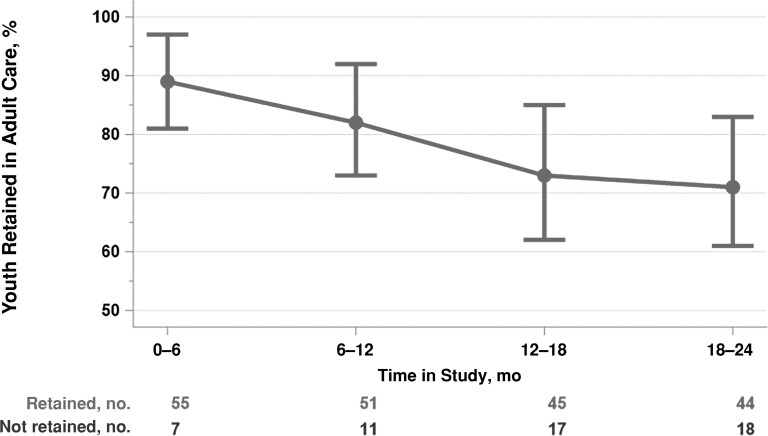
Results: The majority of our cohort (n = 70) was male (88.6%) and black (92.9%) and acquired HIV horizontally (80%). Most of our cohort was linked to adult care by 12 months (84%) after enrollment. Of those who linked to adult care by 12 months, retention rates were 86% (95% confidence interval, 78%-94%) at 6 months, 76% (66%-86%) at 12 months, and 66% (55%-78%) at 18 and 24 months. Once in adult care, the proportion with viral suppression was stable (73% at baseline and 74%, 77%, 67%, and 78% at 6, 12, 18, and 24 months, respectively).
Conclusions: Although most youth successfully linked to adult care, retention rates decreased over the 24-month follow-up period. Rates of viral suppression were stable for those who remained in care. Strategies to support retention in adult care will be critical to optimizing this transition for youth with HIV.
Keywords: HIV care continuum; adolescent health; people with HIV; transition.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. B. C. Z. reports grants or contracts unrelated to this work from National Institute of Mental Health (grant K23MH114771) and participation as a volunteer member of the CombinADO data and safety monitoring board (UH3HD096926; principal investigator, Elaine Abrams). C. d. R. is a scientific advisor for and reports consulting fees from Resverlogix. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Fauci AS, Redfield RR, Sigounas G, Weahkee MD, Giroir BP. Ending the HIV epidemic: a plan for the United States. JAMA 2019; 321:844–5. - PubMed
-
- Centers for Disease Control and Prevention . HIV surveillance report, 2019. Available at:https://www.cdc.gov/hiv/library/reports/hiv-surveillance.html. Accessed 3 June 2022.
-
- Centers for Disease Control and Prevention . Estimated HIV incidence and prevalence in the United States, 2015–2019. Available at:http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html. Accessed 6 June 2022.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
