

Molecular Characterization of BK Polyomavirus Replication in Allogeneic Hematopoietic Cell Transplantation Patients
- PMID: 36409589
- PMCID: PMC10093069
- DOI: 10.1093/infdis/jiac450
Molecular Characterization of BK Polyomavirus Replication in Allogeneic Hematopoietic Cell Transplantation Patients
Abstract
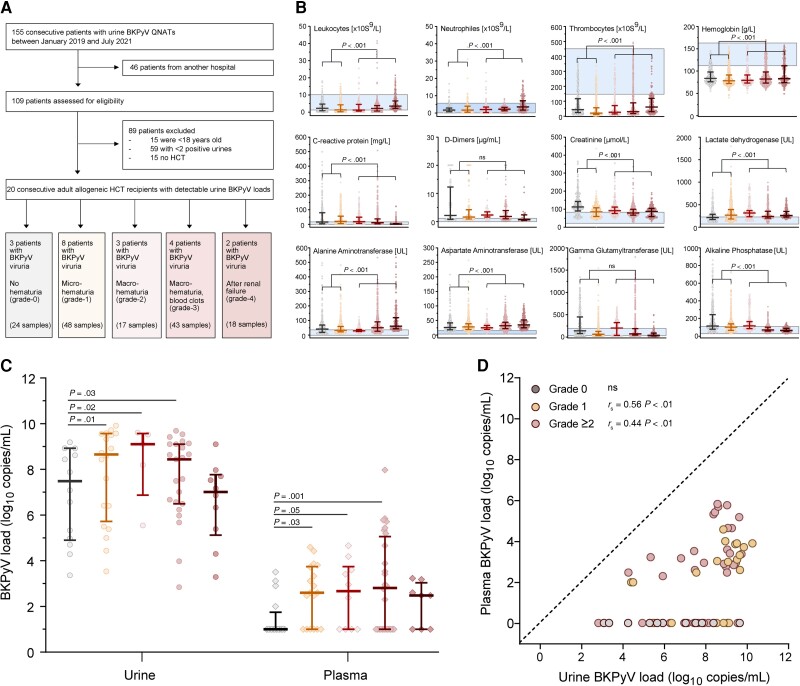
Background: High-level BK polyomavirus (BKPyV) replication in allogeneic hematopoietic cell transplantation (HCT) predicts failing immune control and BKPyV-associated hemorrhagic cystitis.
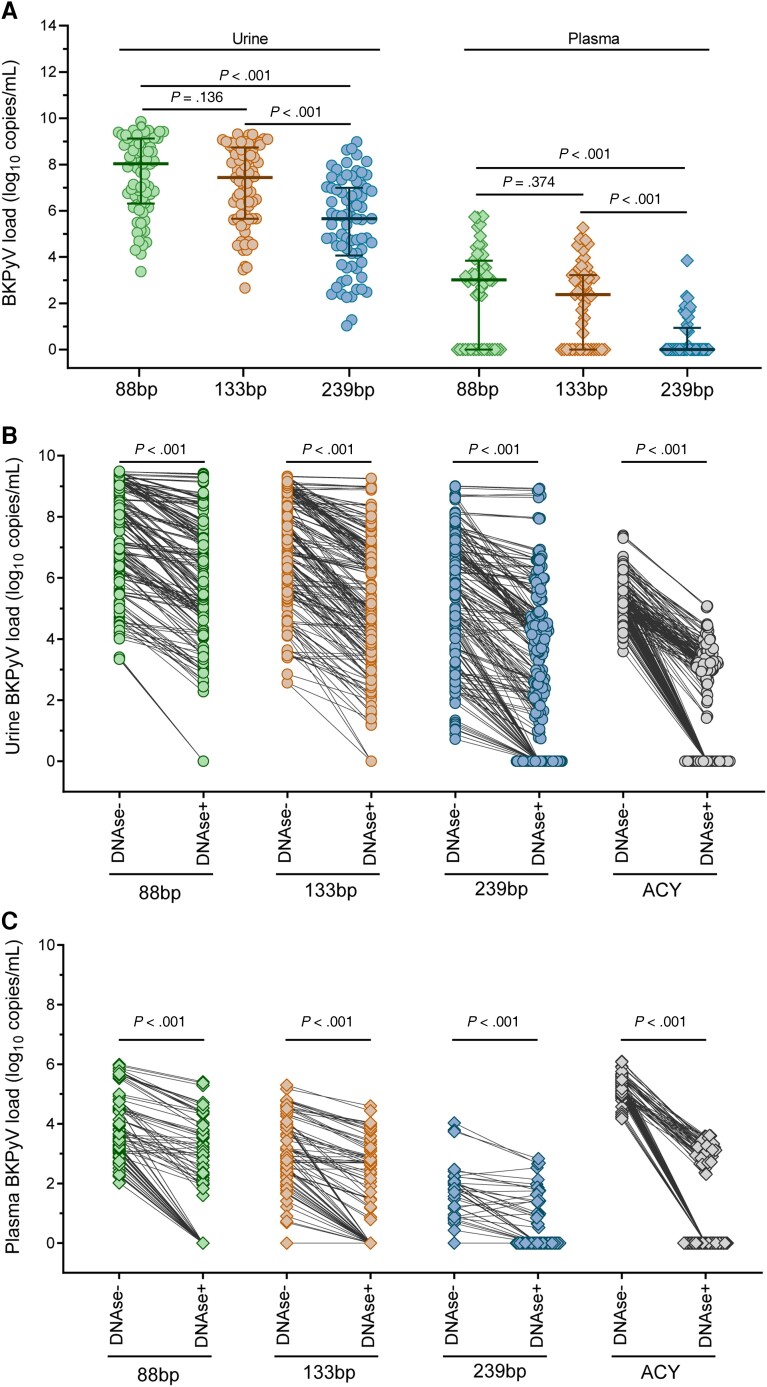
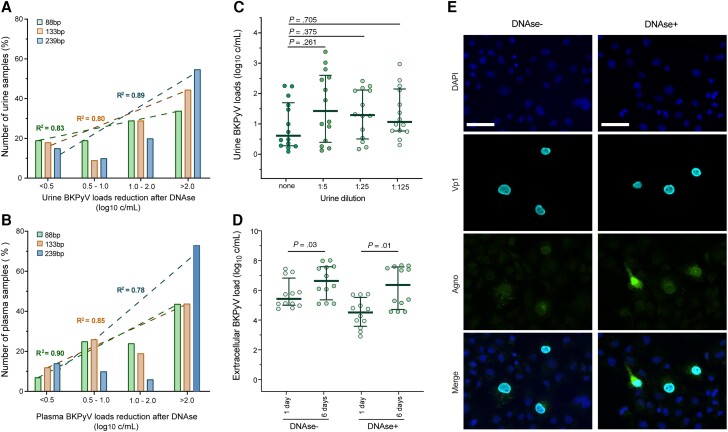
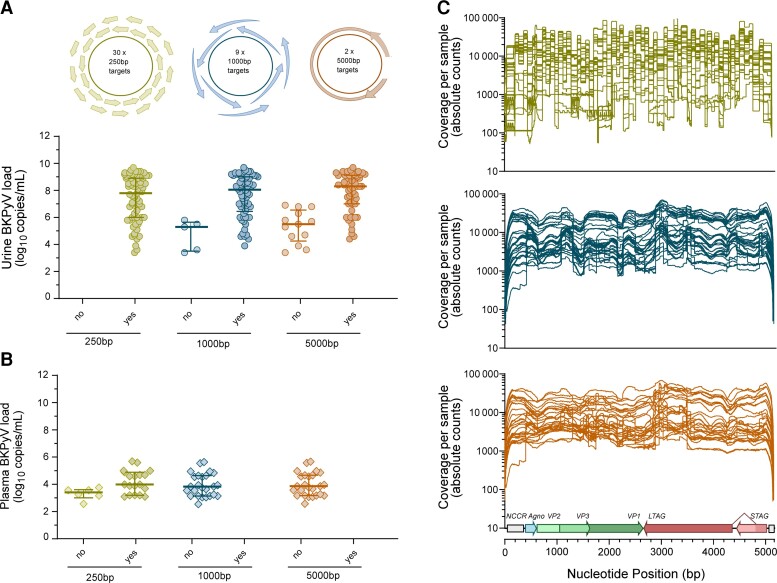
Methods: To identify molecular markers of BKPyV replication and disease, we scrutinized BKPyV DNA-loads in longitudinal urine and plasma pairs from 20 HCT patients using quantitative nucleic acid testing (QNAT), DNase-I treatment prior to QNAT, next-generation sequencing (NGS), and tested cell-mediated immunity.
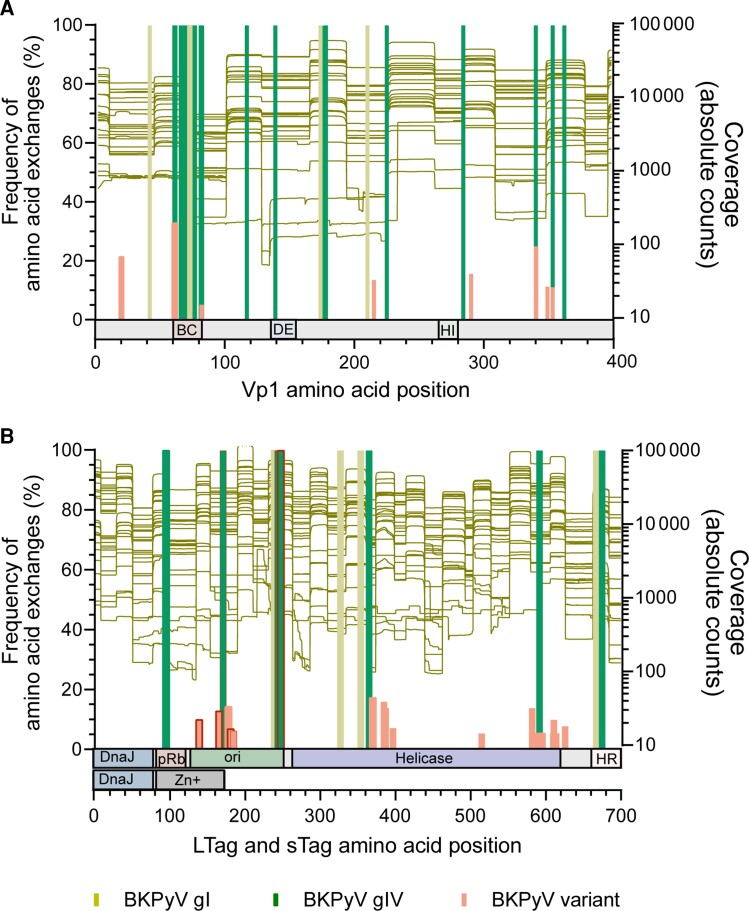
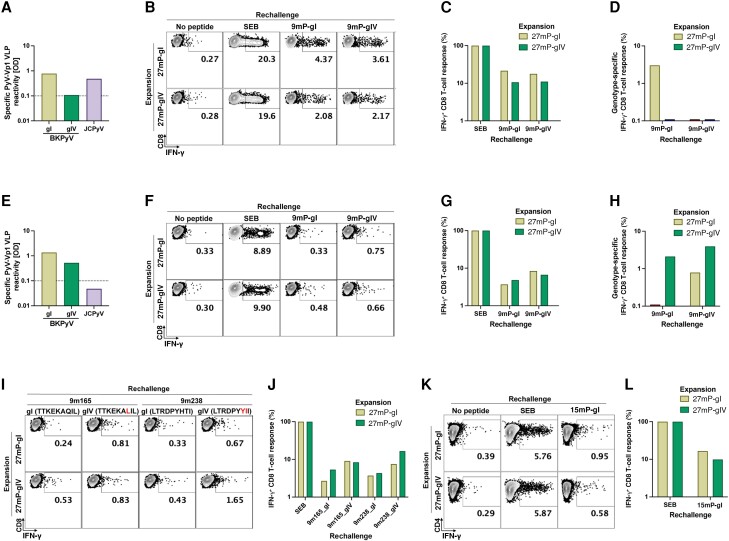
Results: We found that larger QNAT amplicons led to under-quantification and false-negatives results (P < .001). DNase-I reduced urine and plasma BKPyV-loads by >90% (P < .001), indicating non-encapsidated BKPyV genomes. DNase-resistant urine BKPyV-loads remained infectious in cell culture. BKPyV genome fragmentation of ≤250 bp impaired NGS coverage of genetic variation using 1000-bp and 5000-bp amplicons. Conversely, 250-bp amplicons captured viral minority variants. We identified genotype-specific and genotype-independent changes in capsid Vp1 or T-antigen predicted to escape from antibody neutralization or cytotoxic CD8 T-cells, respectively. Genotype-specific changes in immunodominant 9mers were associated with reduced or absent CD8 T-cell responses. Thus, failure to control BKPyV replication in HCT Patients may involve insufficient genotype-specific cytotoxic CD8 T-cell responses, potentially predictable by low neutralizing antibodies as well as genotype-independent immune escape.
Conclusions: Our results provide new insights for patient evaluation and for designing immune protection through neutralizing antibodies, adoptive T-cell therapy, or vaccines.
Keywords: BK polyomavirus; BKPyV; CD8; HCT; LTag; T cell; Vp1; epitope; hematopoietic cell transplantation; hemorrhagic cystitis; immune escape; neutralizing antibody.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. H. H. H. has received speaker honorarium from Gilead, Biotest, and Vera Therapeutics; and served as consultant for Roche, Molecular Partners, Vera Therapeutics, and AiCuris. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed
Figures
References
-
- Graf FE, Hirsch HH. BK polyomavirus after solid organ and hematopoietic cell transplantation: one virus–three diseases. In: Morris MI, Kotton CN, Wolfe C, eds. Emerging transplant infections. Cham, Switzerland: Springer Nature, 2020:1–26.
-
- Cesaro S, Dalianis T, Hanssen Rinaldo C, et al. ECIL guidelines for the prevention, diagnosis and treatment of BK polyomavirus-associated haemorrhagic cystitis in haematopoietic stem cell transplant recipients. J Antimicrob Chemother 2018; 73:12–21. - PubMed
-
- Egli A, Infanti L, Dumoulin A, et al. Prevalence of polyomavirus BK and JC infection and replication in 400 healthy blood donors. J Infect Dis 2009; 199:837–46. - PubMed
-
- Arthur RR, Shah KV, Baust SJ, Santos GW, Saral R. Association of BK viruria with hemorrhagic cystitis in recipients of bone marrow transplants. N Engl J Med 1986; 315:230–4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
