

Time to Renitrogenation After Maximal Denitrogenation in Healthy Volunteers in the Supine and Sitting Positions
- PMID: 36409938
- PMCID: PMC9683758
- DOI: 10.5811/westjem.2022.5.55378
Time to Renitrogenation After Maximal Denitrogenation in Healthy Volunteers in the Supine and Sitting Positions
Abstract
Introduction: Prior to intubation, preoxygenation is performed to denitrogenate the lungs and create an oxygen reservoir. After oxygen is removed, it is unclear whether renitrogenation after preoxygenation occurs faster in the supine vs the sitting position.
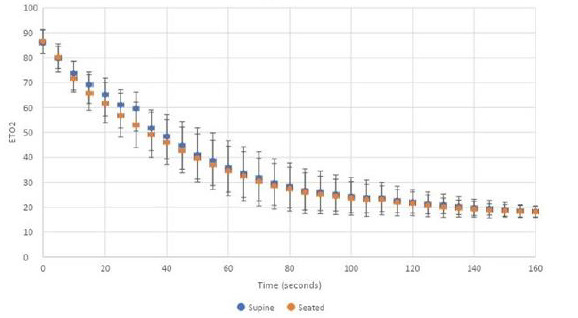
Methods: We enrolled 80 healthy volunteers who underwent two preoxygenation and loss of preoxygenation procedures (one while supine and one while sitting) via bag-valve-mask ventilation with spontaneous breathing. End-tidal oxygen (ETO2) measurements were recorded as fraction of expired oxygen prior to preoxygenation, at the time of adequate preoxygenation (ETO2 >85%), and then every five seconds after the oxygen was removed until the ETO2 values reached their recorded baseline.
Results: The mean ETO2 at completion of preoxygenation was 86% (95% confidence interval 85-88%). Volunteers in both the supine and upright position lost >50% of their denitrogenation in less than 60 seconds. Within 25 seconds, all subjects had an ETO2 of <70%. Complete renitrogenation, defined as return to baseline ETO2, occurred in less than 160 seconds for all volunteers.
Conclusion: Preoxygenation loss, or renitrogenation, occurred rapidly after oxygen removal and was not different in the supine and sitting positions. After maximal denitrogenation in healthy volunteers, renitrogenation occurred rapidly after oxygen removal and was not different in the supine and sitting positions.
Conflict of interest statement
Figures
References
-
- Weingart SD, Levitan RM. Preoxygenation and prevention of desaturation during emergency airway management. Ann Emerg Med. 2012;59(3):165–75. - PubMed
-
- Brown CA, 3rd, Bair AE, Pallin DJ, et al. Techniques, success, and adverse events of emergency department adult intubations. Ann Emerg Med. 2015;65(4):363–70. - PubMed
-
- Tanoubi I, Drolet P, Donati F. Optimizing preoxygenation in adults. Can J Anaesth. 2009;56(6):449–66. - PubMed
-
- Weingart SD, Trueger NS, Wong N, et al. Delayed sequence intubation: a prospective observational study. Ann Emerg Med. 2015;65(4):349–55. - PubMed
-
- Benumof JL. Preoxygenation: best method for both efficacy and efficiency. Anesthesiology. 1999;91(3):603–5. - PubMed