

Multiple sclerosis progression: time for a new mechanism-driven framework
- PMID: 36410373
- PMCID: PMC10463558
- DOI: 10.1016/S1474-4422(22)00289-7
Multiple sclerosis progression: time for a new mechanism-driven framework
Abstract
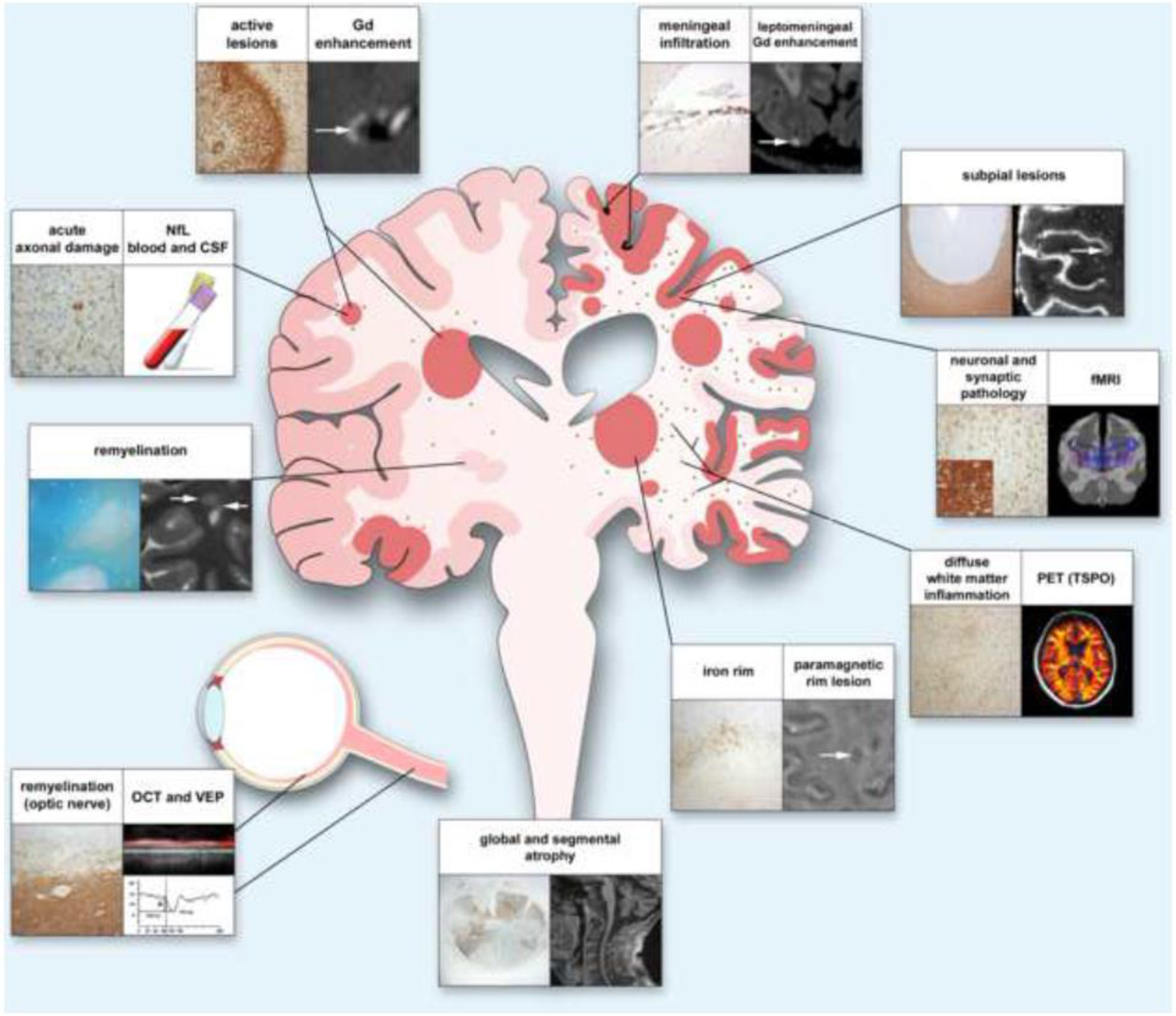
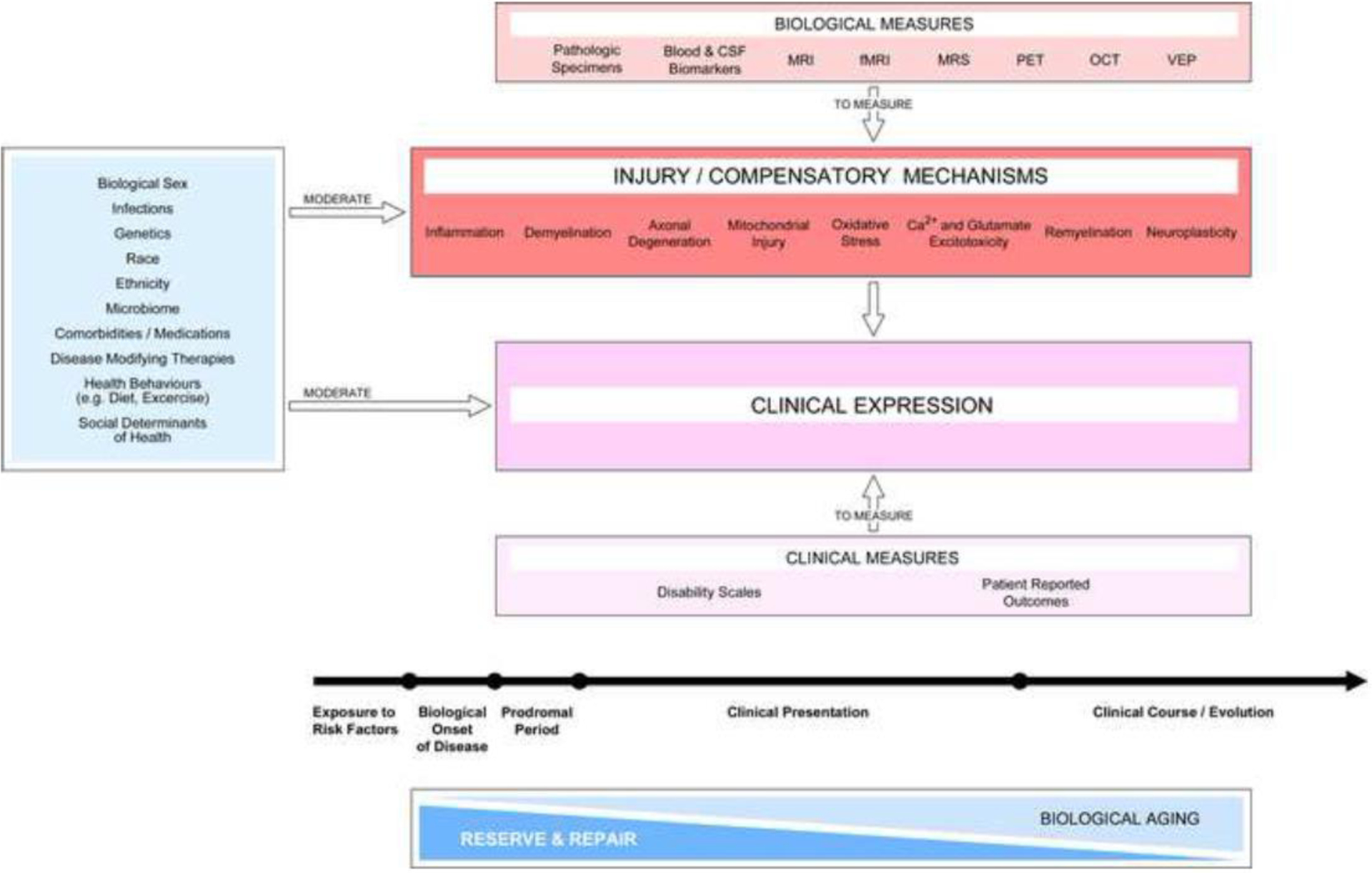
Traditionally, multiple sclerosis has been categorised by distinct clinical descriptors-relapsing-remitting, secondary progressive, and primary progressive-for patient care, research, and regulatory approval of medications. Accumulating evidence suggests that the clinical course of multiple sclerosis is better considered as a continuum, with contributions from concurrent pathophysiological processes that vary across individuals and over time. The apparent evolution to a progressive course reflects a partial shift from predominantly localised acute injury to widespread inflammation and neurodegeneration, coupled with failure of compensatory mechanisms, such as neuroplasticity and remyelination. Ageing increases neural susceptibility to injury and decreases resilience. These observations encourage a new consideration of the course of multiple sclerosis as a spectrum defined by the relative contributions of overlapping pathological and reparative or compensatory processes. New understanding of key mechanisms underlying progression and measures to quantify progressive pathology will potentially have important and beneficial implications for clinical care, treatment targets, and regulatory decision-making.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests TK received research funding from the German Research Foundation, Interdisciplinary Centre for Clinical Studies (IZKF) Münster, National Multiple Sclerosis Society (USA), European Leukodystrophy Association, Progressive MS Alliance, European Commission (H2020-MSCA-ITN-2018), and Novartis; and received compensation for serving on a scientific advisory board (Novartis) and speaker honoraria from Novartis and Roche. MM has received research grants from MAGNIMS-ECTRIMS, Multiple Sclerosis Society UK, and Merck; consulting fees from Ipsen, BMS Celgene, Biogen, Sanofi-Genzyme, Roche, and Merck; honoraria for lectures from Merck, Roche, and Sanofi-Genzyme; and support for attending meetings from Merck, Biogen, and Sanofi-Genzyme. TC is an employee of the National Multiple Sclerosis Society (USA), which is one of the sponsors of the International Advisory Committee on Clinical Trials in Multiple Sclerosis. JAC has received personal compensation for consulting for Biogen, Bristol-Myers Squibb, Convelo, Genentech, Janssen, NervGen, Novartis, and PSI; for speaking for H3 Communications; and for serving as an editor of the Multiple Sclerosis Journal. JC has received grants or contracts from Biogen, Merck and UC San Francisco; and has received payments or honoraria for lectures, speaker bureaus, or presentations from Biogen, Merck, Sanofi Genzyme, Novartis, Bristol-Myers, and Roche; participation on Data Safety Monitoring Boards or Advisory Boards from Novartis, Merck, Sanofi Genzyme, and Biogen. JG has received grant and contract research support from the National Multiple Sclerosis Society (USA), Biogen, and Octave Biosciences; serves on a steering committee for a trial supported by Novartis; has received speaker fees from Alexion and BMS; and served on an advisory board for Genentech. XM received speaking honoraria and travel expenses for participation in scientific meetings; has been a steering committee member of clinical trials or participated in advisory boards of clinical trials with Abbvie, Actelion, Alexion, Biogen, Bristol-Myers Squibb/Celgene, EMD Serono, Genzyme, Hoffmann-La Roche, Sandoz, Immunic, Janssen Pharmaceuticals, Medday, Merck, Mylan, Nervgen, Novartis, Sanofi-Genzyme, Teva Pharmaceuticals, TG Therapeutics, Excemed, Multiple Sclerosis International Federation, and National Multiple Sclerosis Society (USA). RAM receives research funding from Biogen Idec and Roche; and is the chair of the Medical Advisory Committee of the Multiple Sclerosis Society of Canada. VWY is funded by research grants from the Multiple Sclerosis Society of Canada, the Canadian Institutes of Health Research, Canadian Cancer Society, and Genentech; has received speaker honoraria from Biogen, EMD Serono, Novartis, Roche, and Sanofi-Genzyme; and is the recipient of unrestricted educational grants from Biogen, EMD Serono, Novartis, Roche, Sanofi-Genzyme, and Teva Canada to support educational activities of the Alberta MS Network, which he directs. AJT reports personal fees as an editorial board member for The Lancet Neurology receiving a free subscription; is Editor-in-Chief for the Multiple Sclerosis Journal receiving an honorarium from SAGE Publications; receives support from the UCLH NIHR Biomedical Research Centre; and receives support for travel as Chair of the Scientific Advisory Committee and International Progressive MS Alliance from the National MS Society (USA) as member, National Multiple Sclerosis Society (USA) Research Programs Advisory Committee, and as a Board member of the European Charcot Foundation; has received payment in the past 36 months (paid to the UCL) from Eisai and from the German Aerospace Centre, Health Research (ERA-NET NEURON); has received fees or support for travel from Hoffman La Roche, Novartis, and CanProCo SAB; had received honoraria or support for travel from EXCEMED and Almirall; has received support for travel to PACTRIMS and has received support for travel to the Multiple Sclerosis Society of Canada; unpaid roles include as a Guarantor of BRAIN, Trustee of the National Brain Appeal (National Hospital for Neurology and Neurosurgery), and as Chair of the Scientific Ambassadors, ‘STOP MS’ Appeal Board (Multiple Sclerosis Society UK). DSR reports personal fees from Bounds Law Group LLC, grants from Vertex, grants from Sanofi-Genzyme, grants from Abata Therapeutics, outside the submitted work; has a patent system and method of automatically detecting tissue abnormalities (US Patent 9,607,392) issued, a patent method of analysing multisequence MRI data for analysing brain abnormalities in a subject (US Patent 9,888,876) issued, a patent Automatic identification of subjects at risk of multiple sclerosis (US Patent application 16/254,710) issued, and a patent high-resolution cerebrospinal fluid-suppressed T2*-weighted magnetic resonance imaging of cortical lesions (US Patent application 62/838,578) pending.
Figures
Comment in
-
Time to reconsider the classification of multiple sclerosis.Lancet Neurol. 2023 Jan;22(1):6-8. doi: 10.1016/S1474-4422(22)00469-0. Epub 2022 Nov 18. Lancet Neurol. 2023. PMID: 36410374 No abstract available.
References
-
- Olsson T, Barcellos LF, Alfredsson L. Interactions between genetic, lifestyle and environmental risk factors for multiple sclerosis. Nat Rev Neurol 2017; 13(1): 25–36. - PubMed
-
- Lublin FD, Reingold SC. Defining the clinical course of multiple sclerosis: results of an international survey. National Multiple Sclerosis Society (USA) Advisory Committee on Clinical Trials of New Agents in Multiple Sclerosis. Neurology 1996; 46(4): 907–11. - PubMed
-
- Montalban X, Hauser SL, Kappos L, et al. Ocrelizumab versus Placebo in Primary Progressive Multiple Sclerosis. N Engl J Med 2017; 376(3): 209–20. - PubMed
-
- Kappos L, Bar-Or A, Cree BAC, et al. Siponimod versus placebo in secondary progressive multiple sclerosis (EXPAND): a double-blind, randomised, phase 3 study. Lancet 2018; 391(10127): 1263–73. - PubMed
