

Effects of Bardoxolone Methyl in Alport Syndrome
- PMID: 36411058
- PMCID: PMC9718021
- DOI: 10.2215/CJN.02400222
Effects of Bardoxolone Methyl in Alport Syndrome
Abstract
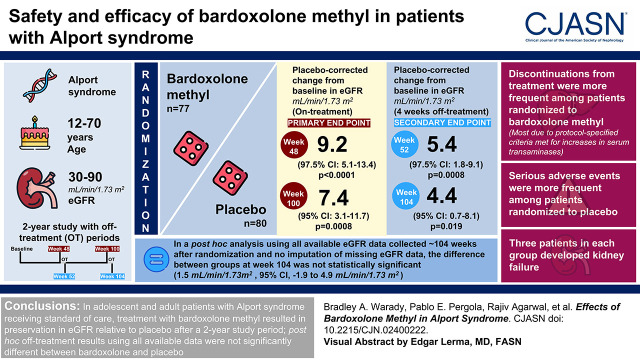
Background and objectives: Alport syndrome is an inherited disease characterized by progressive loss of kidney function. We aimed to evaluate the safety and efficacy of bardoxolone methyl in patients with Alport syndrome.
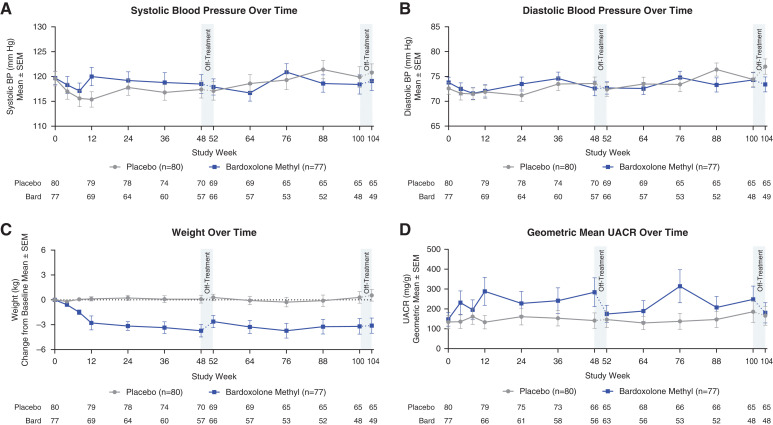
Design, setting, participants, & measurements: We randomly assigned patients with Alport syndrome, ages 12-70 years and eGFR 30-90 ml/min per 1.73 m2, to bardoxolone methyl (n=77) or placebo (n=80). Primary efficacy end points were change from baseline in eGFR at weeks 48 and 100. Key secondary efficacy end points were change from baseline in eGFR at weeks 52 and 104, after an intended 4 weeks off treatment. Safety was assessed by monitoring for adverse events and change from baseline in vital signs, 12-lead electrocardiograms, laboratory measurements (including, but not limited to, aminotransferases, urinary albumin-creatinine ratio, magnesium, and B-type natriuretic peptide), and body weight.
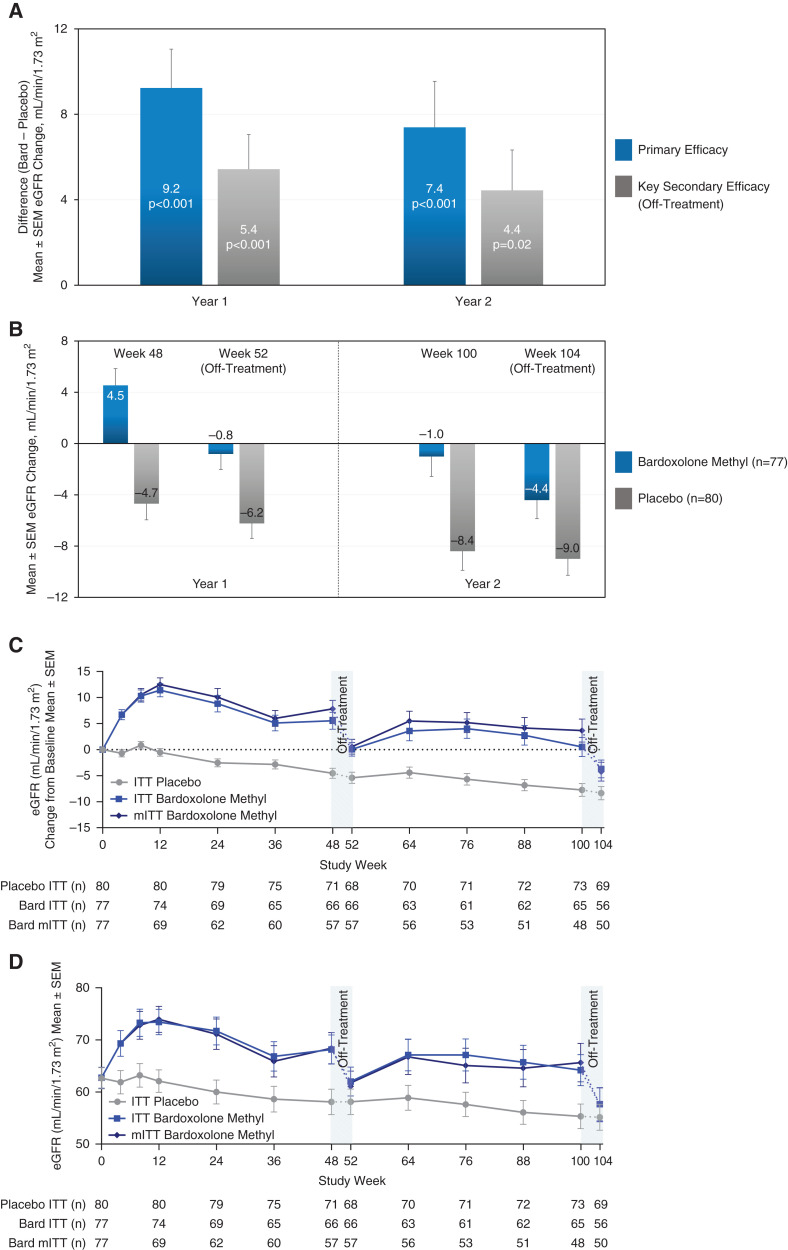
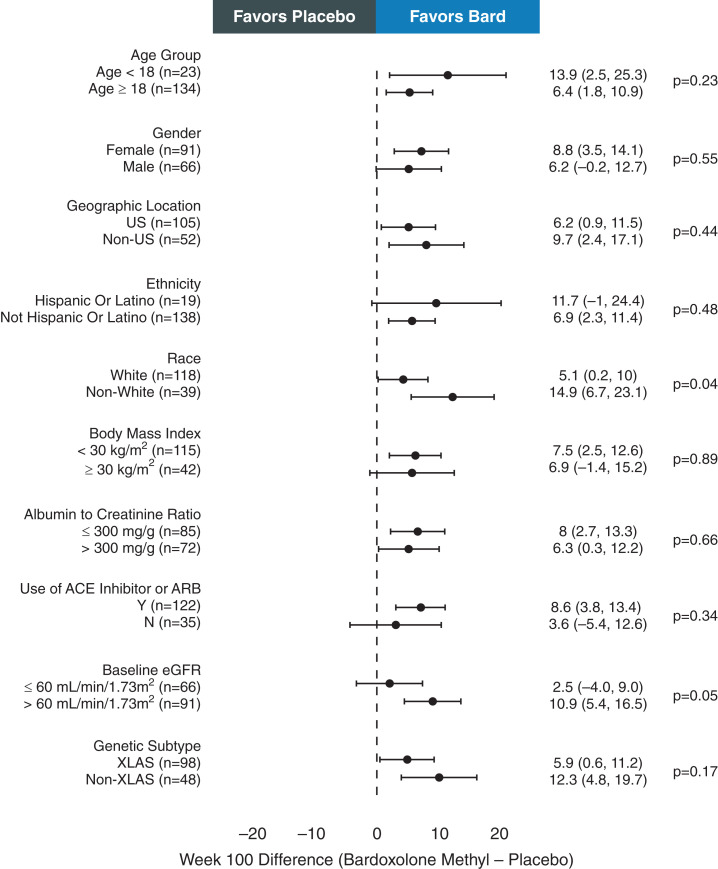
Results: Patients randomized to bardoxolone methyl experienced preservation in eGFR relative to placebo at 48 and 100 weeks (between-group differences: 9.2 [97.5% confidence interval, 5.1 to 13.4; P<0.001] and 7.4 [95% confidence interval, 3.1 to 11.7; P=0.0008] ml/min per 1.73 m2, respectively). After a 4-week off-treatment period, corresponding mean differences in eGFR were 5.4 (97.5% confidence interval, 1.8 to 9.1; P<0.001) and 4.4 (95% confidence interval, 0.7 to 8.1; P=0.02) ml/min per 1.73 m2 at 52 and 104 weeks, respectively. In a post hoc analysis with no imputation of missing eGFR data, the difference at week 104 was not statistically significant (1.5 [95% confidence interval, -1.9 to 4.9] ml/min per 1.73 m2). Discontinuations from treatment were more frequent among patients randomized to bardoxolone methyl; most discontinuations were due to protocol-specified criteria being met for increases in serum transaminases. Serious adverse events were more frequent among patients randomized to placebo. Three patients in each group developed kidney failure.
Conclusions: In adolescent and adult patients with Alport syndrome receiving standard of care, treatment with bardoxolone methyl resulted in preservation in eGFR relative to placebo after a 2-year study period; off-treatment results using all available data were not significantly different.
Clinical trial registry name and registration number: A Phase 2/3 Trial of the Efficacy and Safety of Bardoxolone Methyl in Patients with Alport Syndrome - CARDINAL (CARDINAL), NCT03019185.
Keywords: Alport syndrome; CKD; bardoxolone methyl.
Copyright © 2022 by the American Society of Nephrology.
Figures
Comment in
-
Bardoxolone Methyl for Alport Syndrome: Opportunities and Challenges.Clin J Am Soc Nephrol. 2022 Dec;17(12):1713-1715. doi: 10.2215/CJN.12491022. Epub 2022 Nov 21. Clin J Am Soc Nephrol. 2022. PMID: 36411059 Free PMC article. No abstract available.
References
-
- Kruegel J, Rubel D, Gross O: Alport syndrome--Insights from basic and clinical research. Nat Rev Nephrol 9: 170–178, 2013 - PubMed
-
- Jais JP, Knebelmann B, Giatras I, Marchi M, Rizzoni G, Renieri A, Weber M, Gross O, Netzer KO, Flinter F, Pirson Y, Verellen C, Wieslander J, Persson U, Tryggvason K, Martin P, Hertz JM, Schröder C, Sanak M, Krejcova S, Carvalho MF, Saus J, Antignac C, Smeets H, Gubler MC: X-linked Alport syndrome: Natural history in 195 families and genotype- phenotype correlations in males. J Am Soc Nephrol 11: 649–657, 2000 - PubMed
-
- Jais JP, Knebelmann B, Giatras I, De Marchi M, Rizzoni G, Renieri A, Weber M, Gross O, Netzer KO, Flinter F, Pirson Y, Dahan K, Wieslander J, Persson U, Tryggvason K, Martin P, Hertz JM, Schröder C, Sanak M, Carvalho MF, Saus J, Antignac C, Smeets H, Gubler MC: X-linked Alport syndrome: Natural history and genotype-phenotype correlations in girls and women belonging to 195 families: A “European Community Alport Syndrome Concerted Action” study. J Am Soc Nephrol 14: 2603–2610, 2003 - PubMed
-
- Kamiyoshi N, Nozu K, Fu XJ, Morisada N, Nozu Y, Ye MJ, Imafuku A, Miura K, Yamamura T, Minamikawa S, Shono A, Ninchoji T, Morioka I, Nakanishi K, Yoshikawa N, Kaito H, Iijima K: Genetic, clinical, and pathologic backgrounds of patients with autosomal dominant Alport syndrome. Clin J Am Soc Nephrol 11: 1441–1449, 2016 - PMC - PubMed
-
- Savige J, Gregory M, Gross O, Kashtan C, Ding J, Flinter F: Expert guidelines for the management of Alport syndrome and thin basement membrane nephropathy. J Am Soc Nephrol 24: 364–375, 2013 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
