

Modifiers of the Risk of Diabetes for Long-Term Outcomes After Coronary Revascularization: CREDO-Kyoto PCI/CABG Registry
- PMID: 36411876
- PMCID: PMC9675601
- DOI: 10.1016/j.jacasi.2021.12.012
Modifiers of the Risk of Diabetes for Long-Term Outcomes After Coronary Revascularization: CREDO-Kyoto PCI/CABG Registry
Abstract
Background: Diabetes is a well-known risk factor for adverse outcomes after coronary revascularization.
Objectives: This study sought to determine high-risk subgroups in whom the excess risks of diabetes relative to nondiabetes are particularly prominent and thus may benefit from more aggressive interventions.
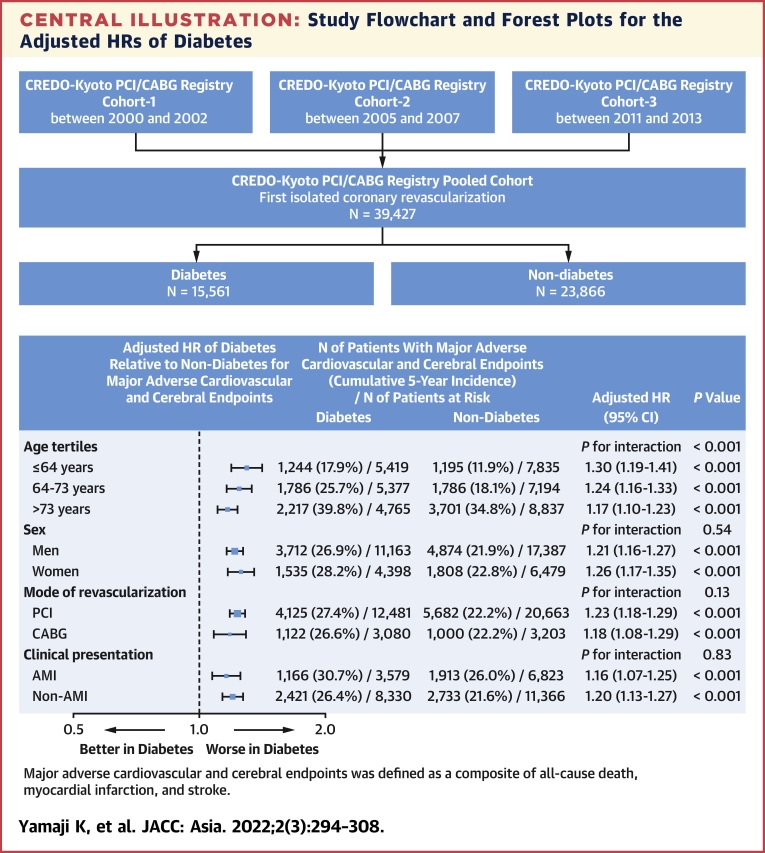
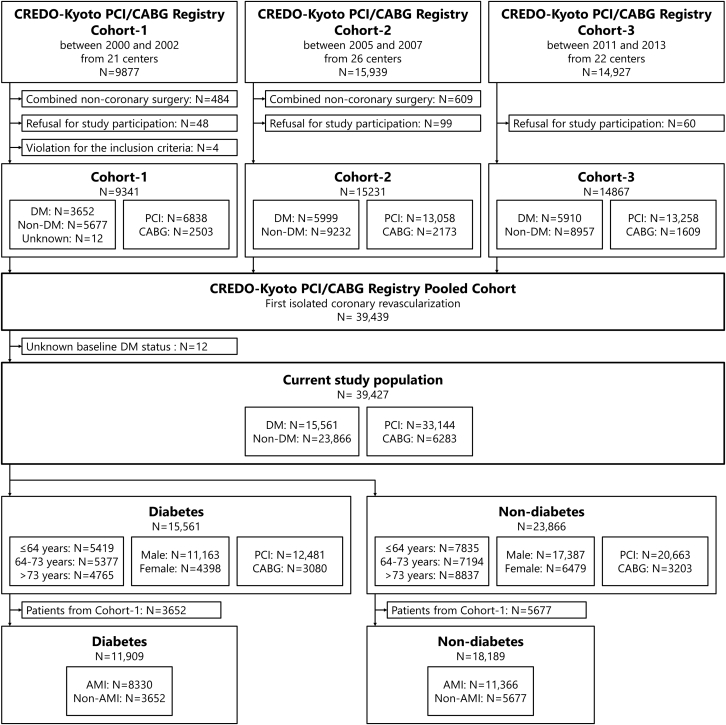
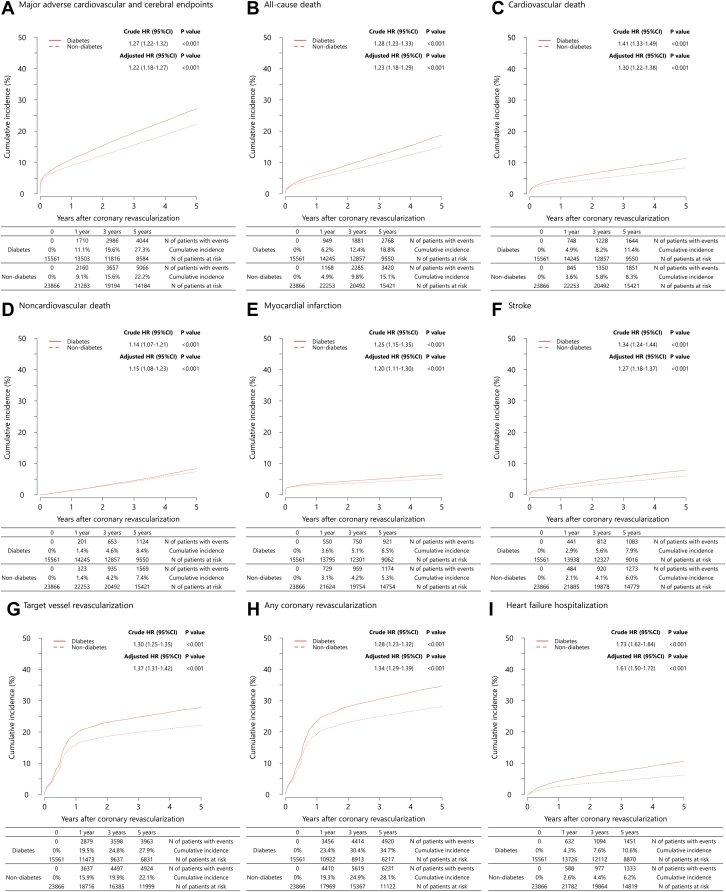
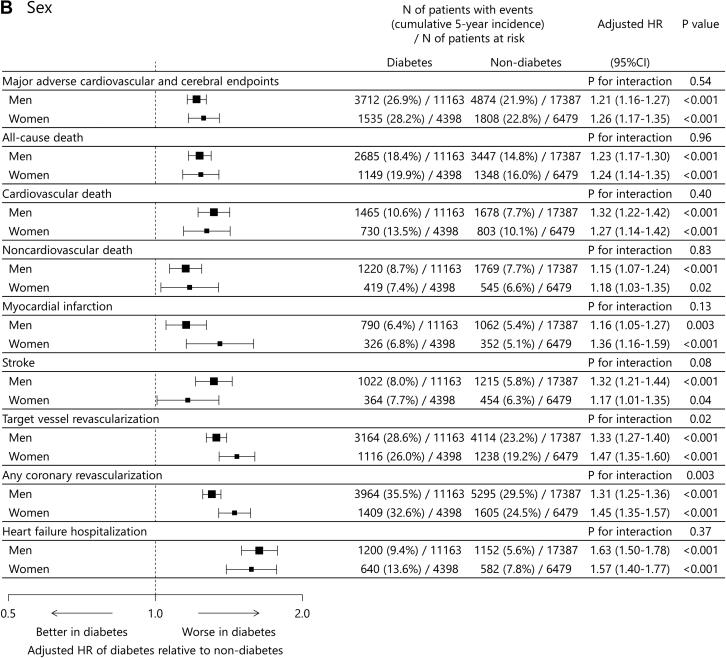
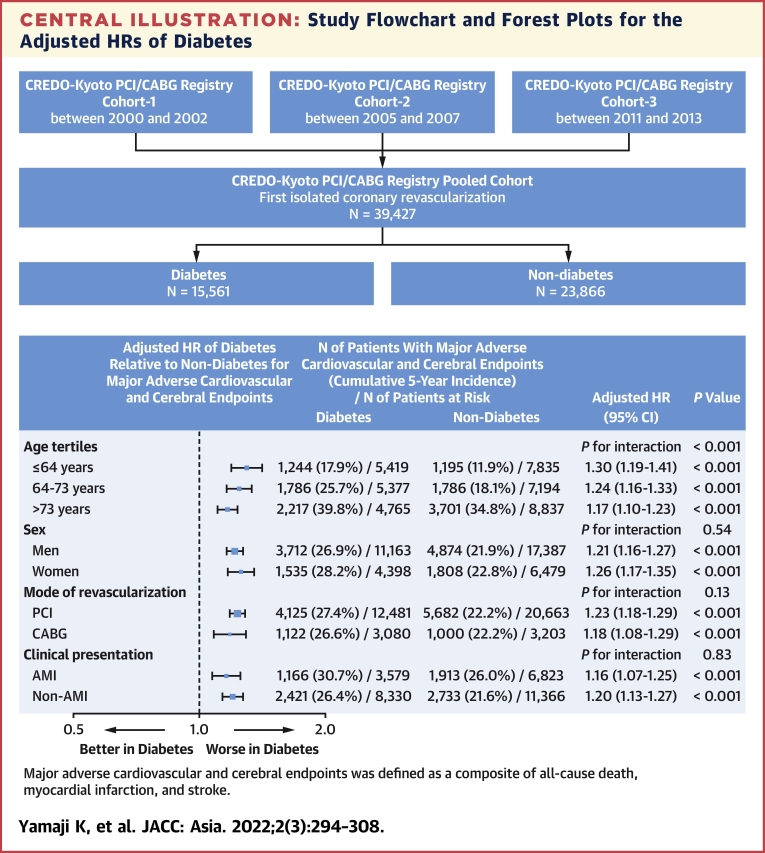
Methods: The study population consisted of 39,427 patients (diabetes: n = 15,561; nondiabetes: n = 23,866) who underwent first percutaneous coronary intervention (n = 33,144) or coronary artery bypass graft (n = 6,283) in the pooled CREDO-Kyoto PCI/CABG (Coronary Revascularization Demonstrating Outcome Study in Kyoto Percutaneous Coronary Intervention/Coronary Artery Bypass Graft) registry. The primary outcome measure was major adverse cardiovascular and cerebral endpoints (MACCE), which was defined as a composite of all-cause death, myocardial infarction, and stroke.
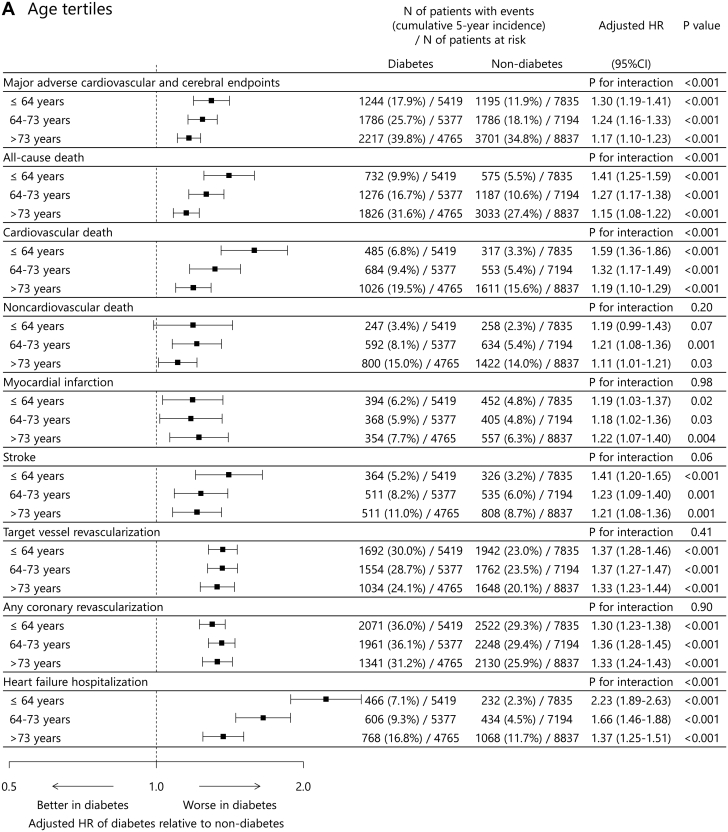
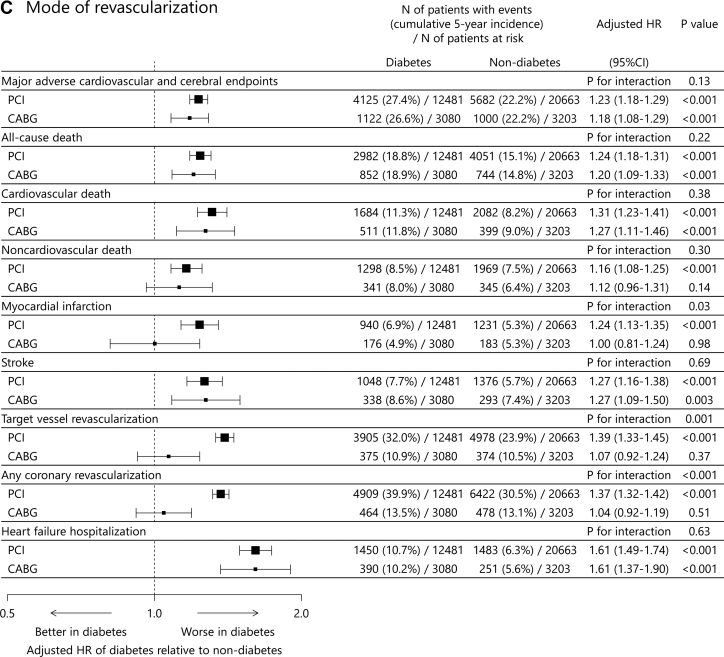
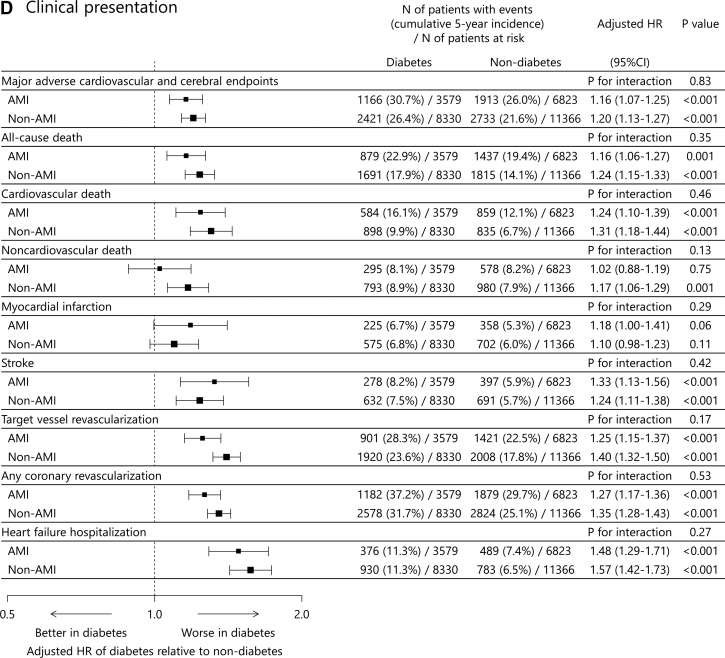
Results: With median follow-up of 5.6 years, diabetes was associated with significantly higher adjusted risks for MACCE. The excess adjusted risks of diabetes relative to nondiabetes for MACCE increased with younger age (≤64 years: adjusted HR: 1.30; 95% CI: 1.19-1.41; P < 0.001; 64-73 years: adjusted HR: 1.24; 95% CI: 1.16-1.33; P < 0.001; >73 years: adjusted HR: 1.17; 95% CI: 1.10-1.23; P < 0.001; P interaction < 0.001), mainly driven by greater excess adjusted mortality risk of diabetes relative to nondiabetes in younger tertile. No significant interaction was observed between adjusted risk of diabetes relative to nondiabetes for MACCE and other subgroups such as sex, mode of revascularization, and clinical presentation of acute myocardial infarction.
Conclusions: The excess risk of diabetes relative to nondiabetes for MACCE was profound in the younger population. This observation suggests more aggressive interventions for secondary prevention in patients with diabetes might be particularly relevant in younger patients.
Keywords: AMI, acute myocardial infarction; CABG, coronary artery bypass graft; MACCE, major adverse cardiovascular and cerebral endpoints; MI, myocardial infarction; PCI, percutaneous coronary intervention; RCT, randomized controlled trial; TVR, target vessel revascularization; coronary artery bypass graft; diabetes; percutaneous coronary intervention.
© 2022 The Authors.
Conflict of interest statement
This study was supported by an educational grant from the Research Institute for Production Development (Kyoto, Japan). Dr Yamaji has received a research grant from Abbott Vascular. Dr Shiomi has received honoraria from Abbott Vascular and Boston Scientific. Dr Morimoto has received lecturer's fees from Bristol-Myers Squibb, Daiichi Sankyo, Japan Lifeline, Kowa, Kyocera, Novartis, and Toray; manuscript fees from Bristol-Myers Squibb and Kowa; and has served on the Advisory Board of Sanofi. Dr Ehara has received honoraria from Abbott Vascular, Bayer, Boston Scientific, Medtronic, and Terumo. Dr Furukawa has received honoraria from Bayer, Kowa, and Sanofi. Dr Nakagawa has received research grants from Abbott Vascular and Boston Scientific; and honoraria from Abbott Vascular, Bayer, and Boston Scientific. Dr Kimura has received a research grant from Abbott Vascular; and honoraria from Astellas, AstraZeneca, Bayer, Boston Scientific, Kowa, and Sanofi. All the other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Tancredi M., Rosengren A., Svensson A.M., et al. Excess mortality among persons with type 2 diabetes. N Engl J Med. 2015;373(18):1720–1732. - PubMed
-
- Rawshani A., Rawshani A., Franzen S., et al. Risk factors, mortality, and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2018;379(7):633–644. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
