

What's new in the pathogeneses and triggering factors of bullous pemphigoid
- PMID: 36412277
- PMCID: PMC10098684
- DOI: 10.1111/1346-8138.16654
What's new in the pathogeneses and triggering factors of bullous pemphigoid
Abstract
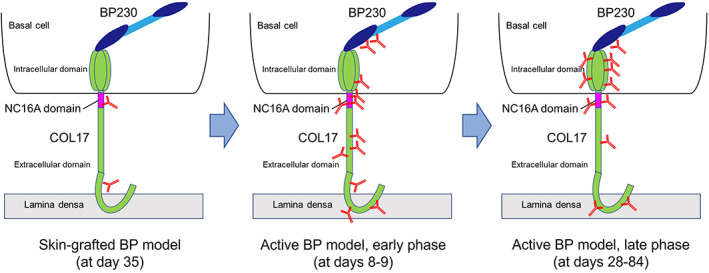
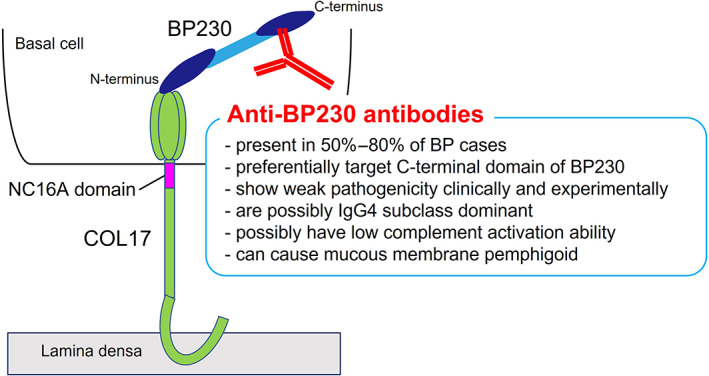
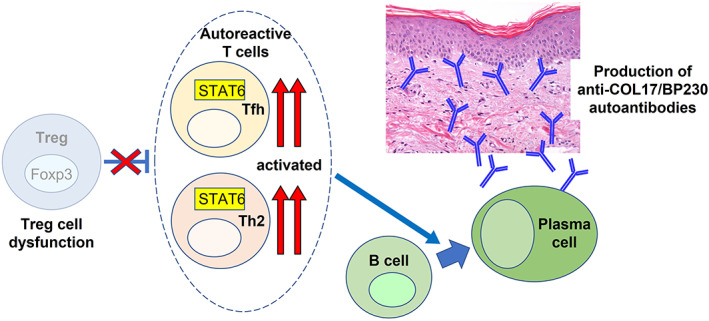
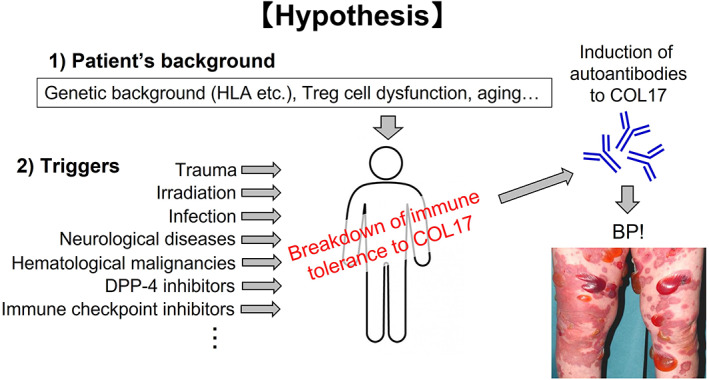
Bullous pemphigoid (BP) is a subepidermal blistering disease induced by autoantibodies to type XVII collagen (COL17, also called BP180) and BP230. Previous studies using patients' samples and animal disease models elucidated the complement-dependent and complement-independent pathways of blister formation, the pathogenic roles of immune cells (T and B cells, macrophages, mast cells, neutrophils, eosinophils), and the pathogenicity of IgE autoantibodies in BP. This review introduces the recent progress on the mechanism behind the epitope-spreading phenomenon in BP, which is considered to be important to understand the chronic and intractable disease course of BP, and the pathogenicity of anti-BP230 autoantibodies, mainly focusing on studies that used active disease models. To clarify the pathogenesis of BP, the mechanism behind the breakdown of immune tolerance to BP antigens should be investigated. Recent studies using various experimental models have revealed important roles for regulatory T cells in the maintenance of self-tolerance to COL17 and BP230 as well as in the suppression of inflammation triggered by the binding of antibodies to COL17. Notably, physical stresses such as trauma, thermal burns, bone fractures, irradiation and ultraviolet exposure, some pathologic conditions such as neurological diseases and hematological malignancies, and the use of dipeptidyl peptidase-IV inhibitors and immune checkpoint inhibitors have been reported as triggering factors for BP. These factors and certain underlying conditions such as genetic background, regulatory T-cell dysfunction or aging might synergistically affect some individuals and eventually induce BP. Further studies on the breakdown of self-tolerance and on the identification of key molecules that are relevant to blister formation and inflammation may expand our understanding of BP's etiology and may lead to the development of novel therapeutic approaches.
Keywords: BP180; BP230; epitope spreading; immune checkpoint inhibitor; regulatory T cell.
© 2022 The Author. The Journal of Dermatology published by John Wiley & Sons Australia, Ltd on behalf of Japanese Dermatological Association.
Conflict of interest statement
The authors declare that we have no conflicts of interest.
Figures
References
-
- Ujiie H, Iwata H, Yamagami J, Nakama T, Aoyama Y, Ikeda S, et al. Japanese guidelines for the management of pemphigoid (including epidermolysis bullosa acquisita). J Dermatol. 2019;46:1102–35. - PubMed
-
- Schmidt E, Zillikens D. Pemphigoid diseases. Lancet. 2013;381:320–32. - PubMed
-
- Diaz LA, Ratrie H, Saunders WS, Futamura S, Squiquera HL, Anhalt GJ, et al. Isolation of a human epidermal cDNA corresponding to the 180‐kD autoantigen recognized by bullous pemphigoid and herpes gestationis sera. Immunolocalization of this protein to the hemidesmosome. J Clin Invest. 1990;86:1088–94. - PMC - PubMed
-
- Giudice GJ, Emery DJ, Diaz LA. Cloning and primary structural analysis of the bullous pemphigoid autoantigen BP180. J Invest Dermatol. 1992;99:243–50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
