

Fading of brain network fingerprint in Parkinson's disease predicts motor clinical impairment
- PMID: 36413043
- PMCID: PMC9875937
- DOI: 10.1002/hbm.26156
Fading of brain network fingerprint in Parkinson's disease predicts motor clinical impairment
Abstract
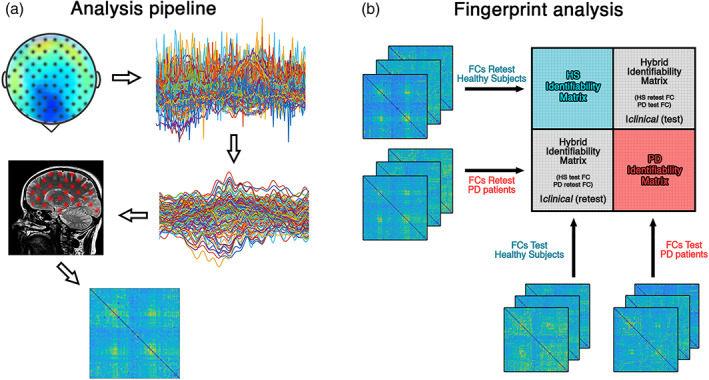
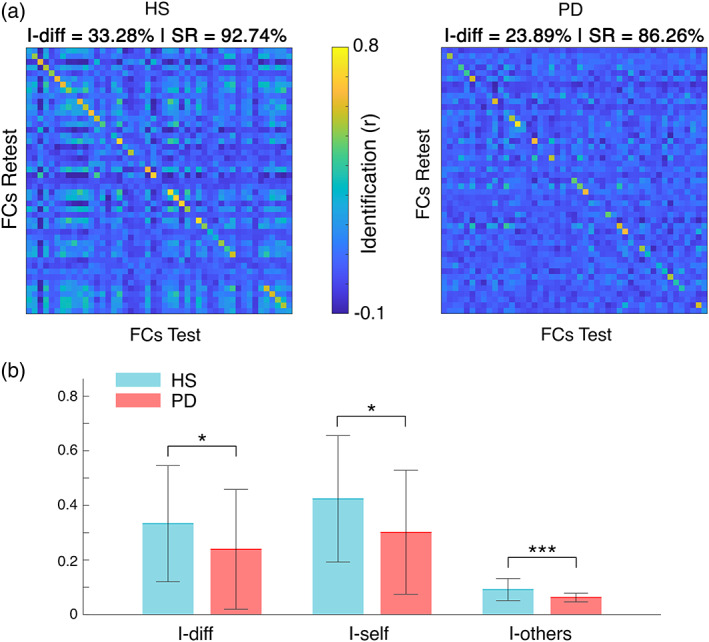
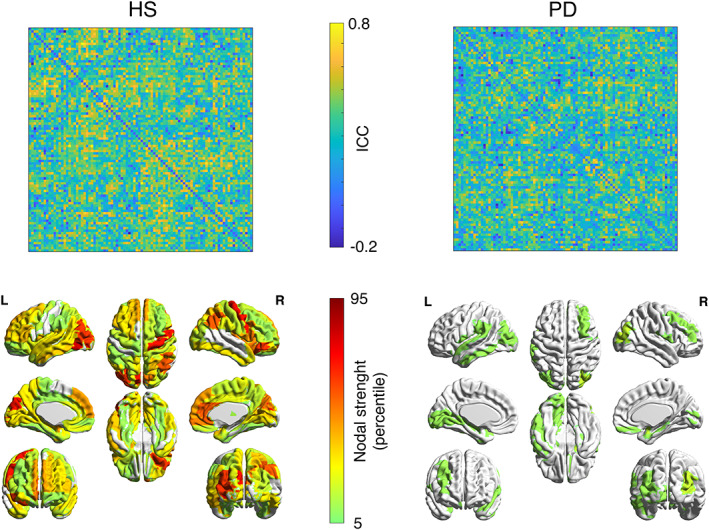
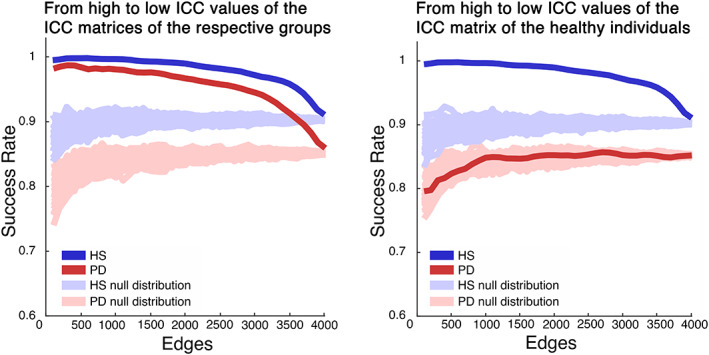
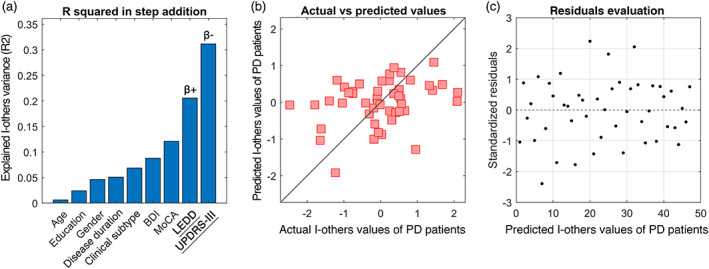
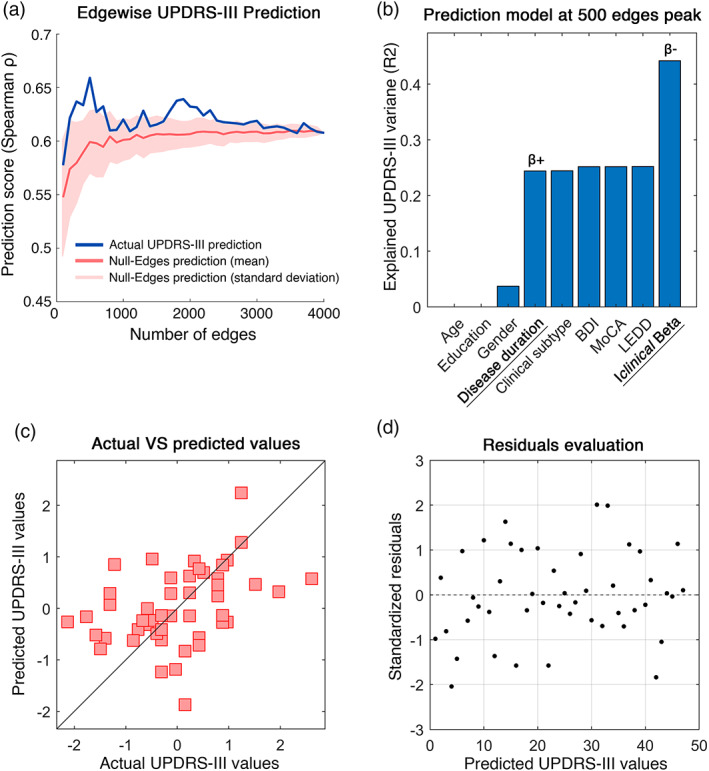
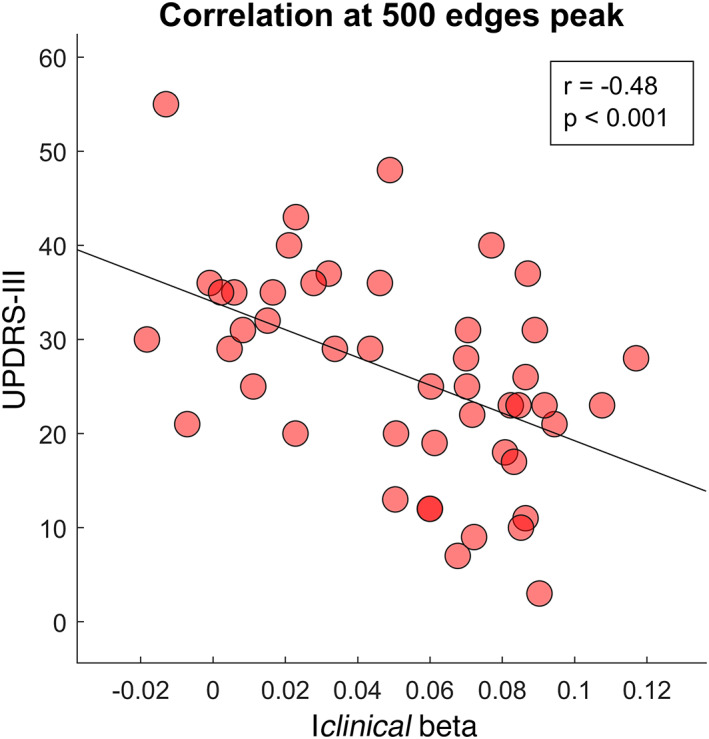
The clinical connectome fingerprint (CCF) was recently introduced as a way to assess brain dynamics. It is an approach able to recognize individuals, based on the brain network. It showed its applicability providing network features used to predict the cognitive decline in preclinical Alzheimer's disease. In this article, we explore the performance of CCF in 47 Parkinson's disease (PD) patients and 47 healthy controls, under the hypothesis that patients would show reduced identifiability as compared to controls, and that such reduction could be used to predict motor impairment. We used source-reconstructed magnetoencephalography signals to build two functional connectomes for 47 patients with PD and 47 healthy controls. Then, exploiting the two connectomes per individual, we investigated the identifiability characteristics of each subject in each group. We observed reduced identifiability in patients compared to healthy individuals in the beta band. Furthermore, we found that the reduction in identifiability was proportional to the motor impairment, assessed through the Unified Parkinson's Disease Rating Scale, and, interestingly, able to predict it (at the subject level), through a cross-validated regression model. Along with previous evidence, this article shows that CCF captures disrupted dynamics in neurodegenerative diseases and is particularly effective in predicting motor clinical impairment in PD.
Keywords: Parkinson's disease; brain fingerprint; brain network; clinical connectome fingerprint; magnetoencephalography; motor impairment; neurodegenerative disease.
© 2022 The Authors. Human Brain Mapping published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflict of interests.
Figures
Similar articles
-
The progressive loss of brain network fingerprints in Amyotrophic Lateral Sclerosis predicts clinical impairment.Neuroimage Clin. 2022;35:103095. doi: 10.1016/j.nicl.2022.103095. Epub 2022 Jun 23. Neuroimage Clin. 2022. PMID: 35764029 Free PMC article.
-
Reduced clinical connectome fingerprinting in multiple sclerosis predicts fatigue severity.Neuroimage Clin. 2023;39:103464. doi: 10.1016/j.nicl.2023.103464. Epub 2023 Jun 28. Neuroimage Clin. 2023. PMID: 37399676 Free PMC article.
-
Brain Networks and Cognitive Impairment in Parkinson's Disease.Brain Connect. 2022 Jun;12(5):465-475. doi: 10.1089/brain.2020.0985. Epub 2021 Sep 8. Brain Connect. 2022. PMID: 34269602
-
A systematic review of MEG-based studies in Parkinson's disease: The motor system and beyond.Hum Brain Mapp. 2019 Jun 15;40(9):2827-2848. doi: 10.1002/hbm.24562. Epub 2019 Mar 7. Hum Brain Mapp. 2019. PMID: 30843285 Free PMC article.
-
Neural Correlates of Cognitive Impairment in Parkinson's Disease: A Review of Structural MRI Findings.Int Rev Neurobiol. 2019;144:1-28. doi: 10.1016/bs.irn.2018.09.009. Epub 2018 Oct 16. Int Rev Neurobiol. 2019. PMID: 30638452 Review.
Cited by
-
Brain flexibility increases during the peri-ovulatory phase as compared to early follicular phase of the menstrual cycle.Sci Rep. 2024 Jan 23;14(1):1976. doi: 10.1038/s41598-023-49588-y. Sci Rep. 2024. PMID: 38263324 Free PMC article.
-
Uncovering longitudinal changes in the brain functional connectome along the migraine cycle: a multilevel clinical connectome fingerprinting framework.J Headache Pain. 2025 Feb 10;26(1):29. doi: 10.1186/s10194-025-01969-6. J Headache Pain. 2025. PMID: 39930372 Free PMC article.
-
Multiplexity of human brain oscillations as a personal brain signature.Hum Brain Mapp. 2023 Dec 1;44(17):5624-5640. doi: 10.1002/hbm.26466. Epub 2023 Sep 5. Hum Brain Mapp. 2023. PMID: 37668332 Free PMC article.
-
Kinematic network of joint motion provides insight on gait coordination: An observational study on Parkinson's disease.Heliyon. 2024 Aug 3;10(15):e35751. doi: 10.1016/j.heliyon.2024.e35751. eCollection 2024 Aug 15. Heliyon. 2024. PMID: 39170156 Free PMC article.
-
Brain fingerprint and subjective mood state across the menstrual cycle.Front Neurosci. 2024 Dec 6;18:1432218. doi: 10.3389/fnins.2024.1432218. eCollection 2024. Front Neurosci. 2024. PMID: 39712222 Free PMC article.
References
-
- Balestrino, R. , & Schapira, A. H. V. (2020). Parkinson disease. European Journal of Neurology, 27(1), 27–42. - PubMed
-
- Barbati, G. , Porcaro, C. , Zappasodi, F. , Rossini, P. M. , & Tecchio, F. (2004). Optimization of an independent component analysis approach for artifact identification and removal in magnetoencephalographic signals. Clinical Neurophysiology, 115(5), 1220–1232. - PubMed
-
- Baselice, F. , Sorriso, A. , Rucco, R. , & Sorrentino, P. (2019). Phase linearity measurement: A novel index for brain functional connectivity. IEEE Transactions on Medical Imaging, 38(4), 873–882. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
