

Assessing the Impact of Prophylactic Eculizumab on Renal Graft Survival in Atypical Hemolytic Uremic Syndrome
- PMID: 36413152
- PMCID: PMC10065821
- DOI: 10.1097/TP.0000000000004355
Assessing the Impact of Prophylactic Eculizumab on Renal Graft Survival in Atypical Hemolytic Uremic Syndrome
Abstract
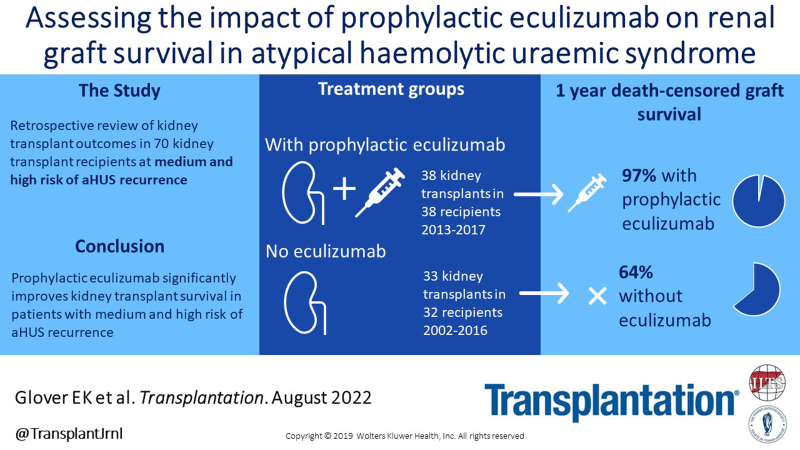
Background: Atypical hemolytic uremic syndrome (aHUS) is a rare cause of end-stage kidney disease and associated with poor outcomes after kidney transplantation from early disease recurrence. Prophylactic eculizumab treatment at the time of transplantation is used in selected patients with aHUS. We report a retrospective case note review describing transplant outcomes in patients with aHUS transplanted between 1978 and 2017, including those patients treated with eculizumab.
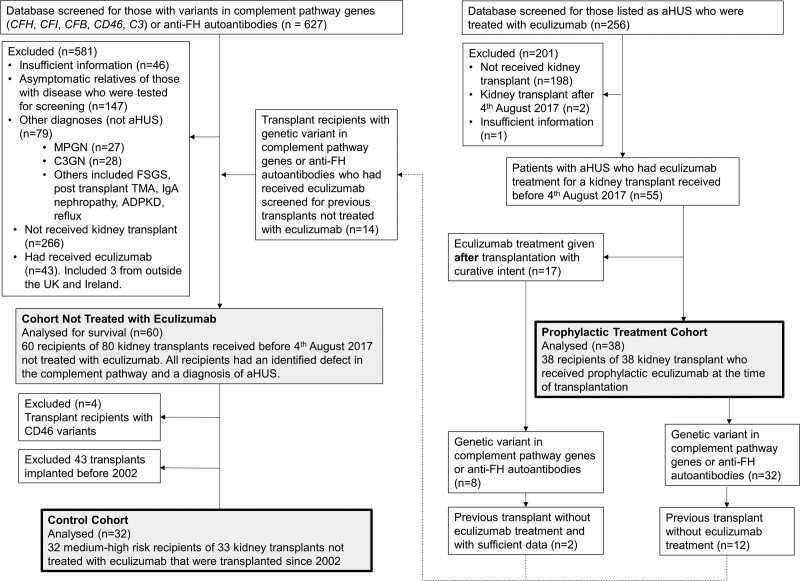
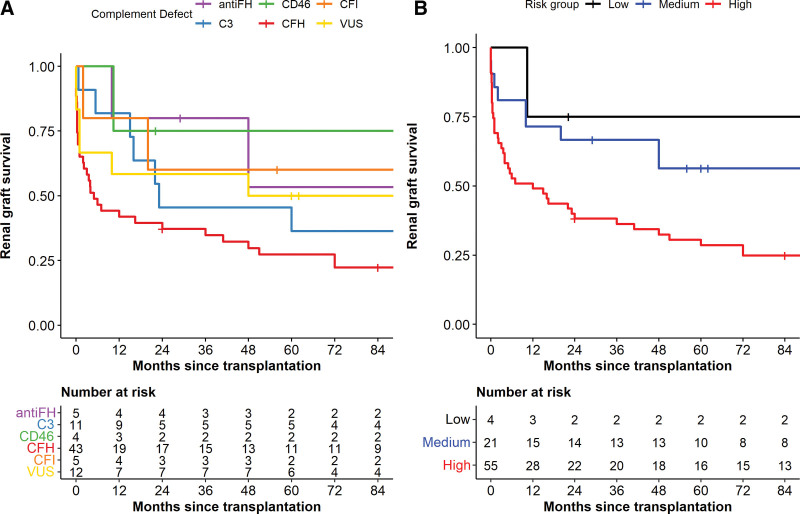
Methods: The National Renal Complement Therapeutics Centre database identified 118 kidney transplants in 86 recipients who had a confirmed diagnosis of aHUS. Thirty-eight kidney transplants were performed in 38 recipients who received prophylactic eculizumab. The cohort not treated with eculizumab comprised 80 transplants in 60 recipients and was refined to produce a comparable cohort of 33 transplants in 32 medium and high-risk recipients implanted since 2002. Complement pathway genetic screening was performed. Graft survival was censored for graft function at last follow-up or patient death. Graft survival without eculizumab treatment is described by complement defect status and by Kidney Disease: Improving Global Outcomes risk stratification.
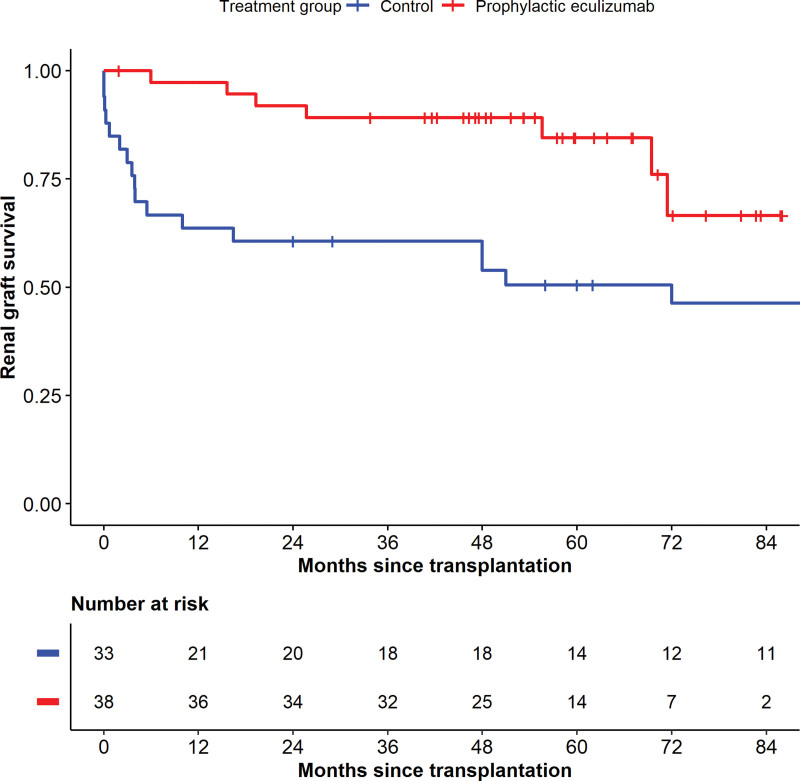
Results: Prophylactic eculizumab treatment improved renal allograft survival ( P = 0.006) in medium and high-risk recipients with 1-y survival of 97% versus 64% in untreated patients. Our data supports the risk stratification advised by Kidney Disease: Improving Global Outcomes.
Conclusions: Prophylactic eculizumab treatment dramatically improves graft survival making transplantation a viable therapeutic option in aHUS.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc.
Figures
References
-
- Goodship TH, Cook HT, Fakhouri F, et al. ; Conference Participants. Atypical hemolytic uremic syndrome and C3 glomerulopathy: conclusions from a “Kidney Disease: Improving Global Outcomes” (KDIGO) Controversies Conference. Kidney Int. 2017;91:539–551. - PubMed
-
- Warwicker P, Goodship TH, Donne RL, et al. . Genetic studies into inherited and sporadic hemolytic uremic syndrome. Kidney Int. 1998;53:836–844. - PubMed
-
- Legendre CM, Licht C, Muus P, et al. . Terminal complement inhibitor eculizumab in atypical hemolytic-uremic syndrome. N Engl J Med. 2013;368:2169–2181. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
