A phase I/II study on intracerebroventricular tralesinidase alfa in patients with Sanfilippo syndrome type B
- PMID: 36413418
- PMCID: PMC9843052
- DOI: 10.1172/JCI165076
A phase I/II study on intracerebroventricular tralesinidase alfa in patients with Sanfilippo syndrome type B
Abstract
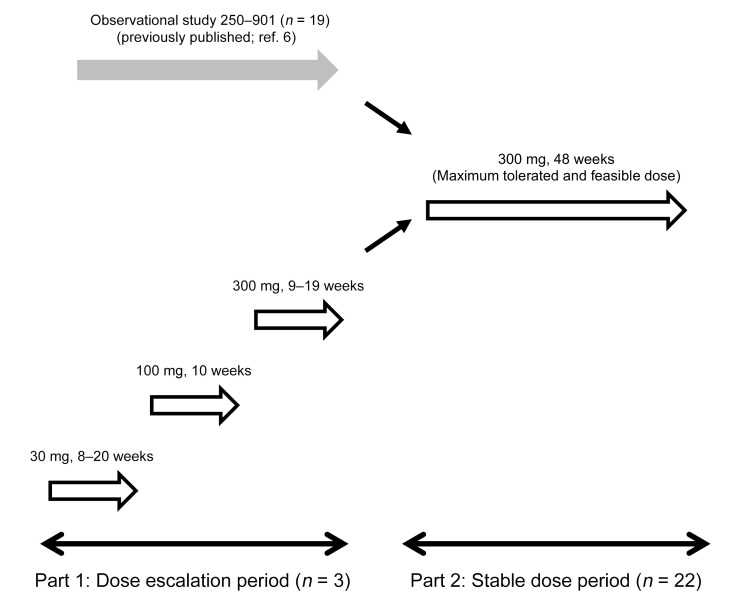
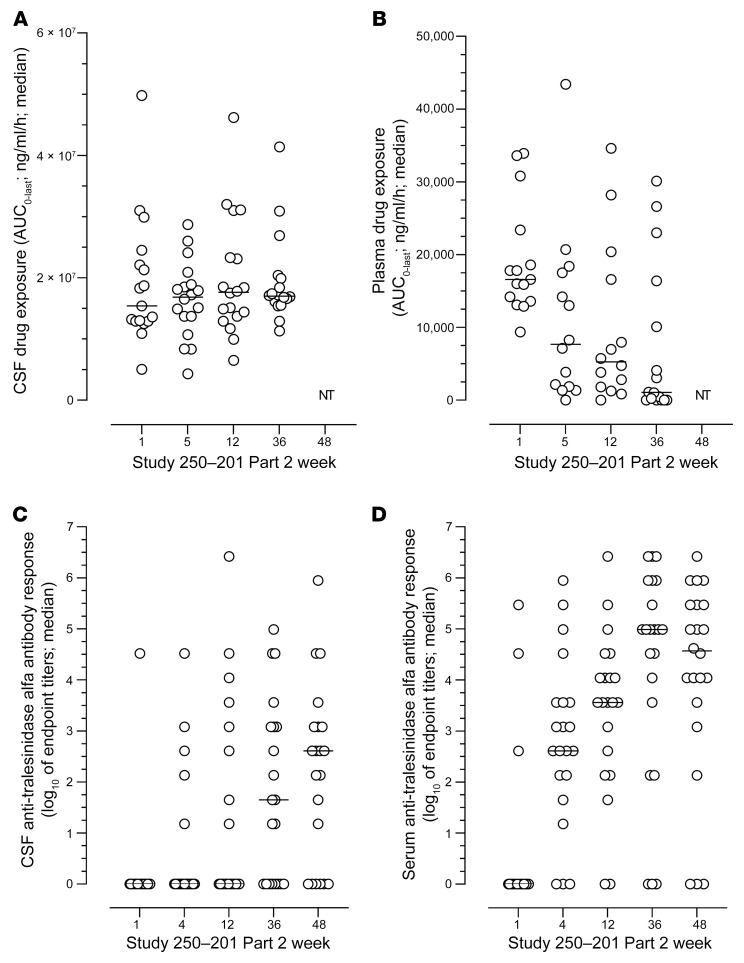
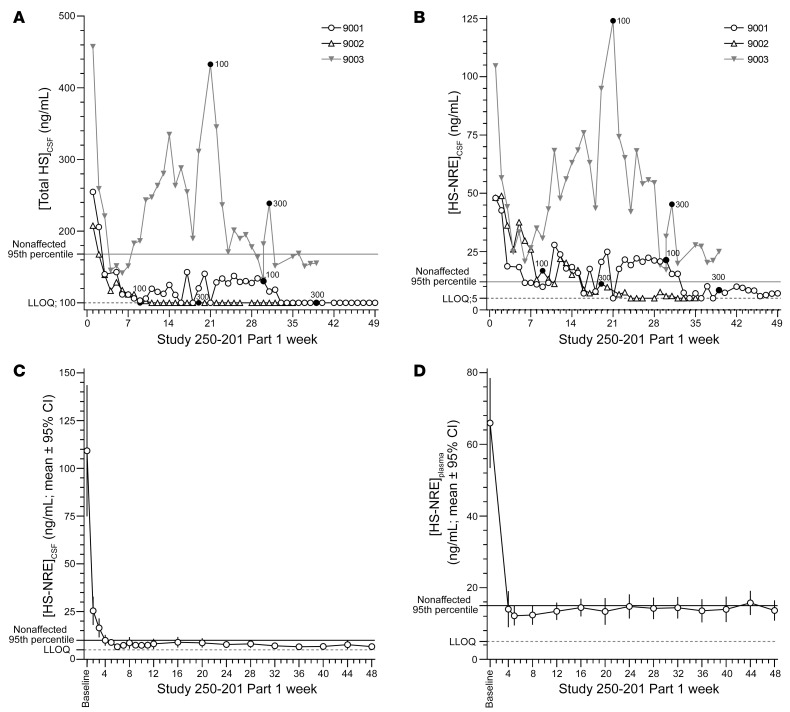
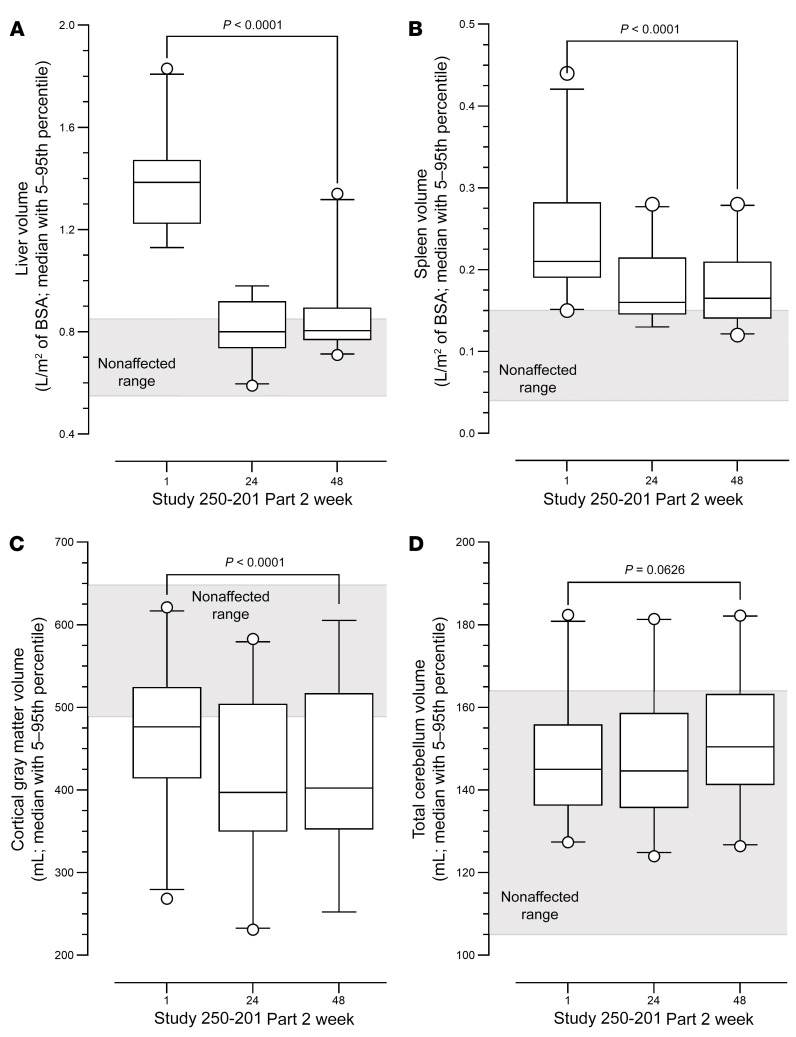
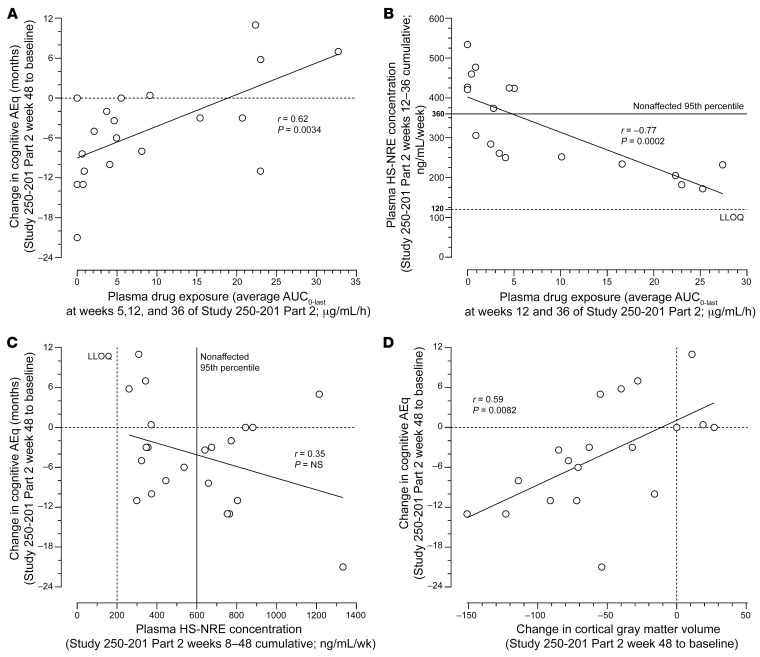
BackgroundSanfilippo type B is a mucopolysaccharidosis (MPS) with a major neuronopathic component characterized by heparan sulfate (HS) accumulation due to mutations in the NAGLU gene encoding alfa-N-acetyl-glucosaminidase. Enzyme replacement therapy for neuronopathic MPS requires efficient enzyme delivery throughout the brain in order to normalize HS levels, prevent brain atrophy, and potentially delay cognitive decline.MethodsIn this phase I/II open-label study, patients with MPS type IIIB (n = 22) were treated with tralesinidase alfa administered i.c.v. The patients were monitored for drug exposure; total HS and HS nonreducing end (HS-NRE) levels in both cerebrospinal fluid (CSF) and plasma; anti-drug antibody response; brain, spleen, and liver volumes as measured by MRI; and cognitive development as measured by age-equivalent (AEq) scores.ResultsIn the Part 1 dose escalation (30, 100, and 300 mg) phase, a 300 mg dose of tralesinidase alfa was necessary to achieve normalization of HS and HS-NRE levels in the CSF and plasma. In Part 2, 300 mg tralesinidase alfa sustained HS and HS-NRE normalization in the CSF and stabilized cortical gray matter volume (CGMV) over 48 weeks of treatment. Resolution of hepatomegaly and a reduction in spleen volume were observed in most patients. Significant correlations were also established between the change in cognitive AEq score and plasma drug exposure, plasma HS-NRE levels, and CGMV.ConclusionAdministration of tralesinidase alfa i.c.v. effectively normalized HS and HS-NRE levels as a prerequisite for clinical efficacy. Peripheral drug exposure data suggest a role for the glymphatic system in altering tralesinidase alfa efficacy.Trial registrationClinicaltrials.gov NCT02754076.FUNDINGBioMarin Pharmaceutical Inc. and Allievex Corporation.
Keywords: Neurological disorders; Neuroscience.
Conflict of interest statement
Figures