

Does gabapentin provide benefit for patients with knee OA? A benefit-harm and cost-effectiveness analysis
- PMID: 36414225
- PMCID: PMC9892279
- DOI: 10.1016/j.joca.2022.07.013
Does gabapentin provide benefit for patients with knee OA? A benefit-harm and cost-effectiveness analysis
Abstract
Objective: Gabapentin can treat neuropathic pain syndromes and has increasingly been prescribed to treat nociplastic pain. Some patients with knee osteoarthritis (OA) suffer from both nociceptive and nociplastic pain. We examined the cost-effectiveness of adding gabapentin to knee OA care.
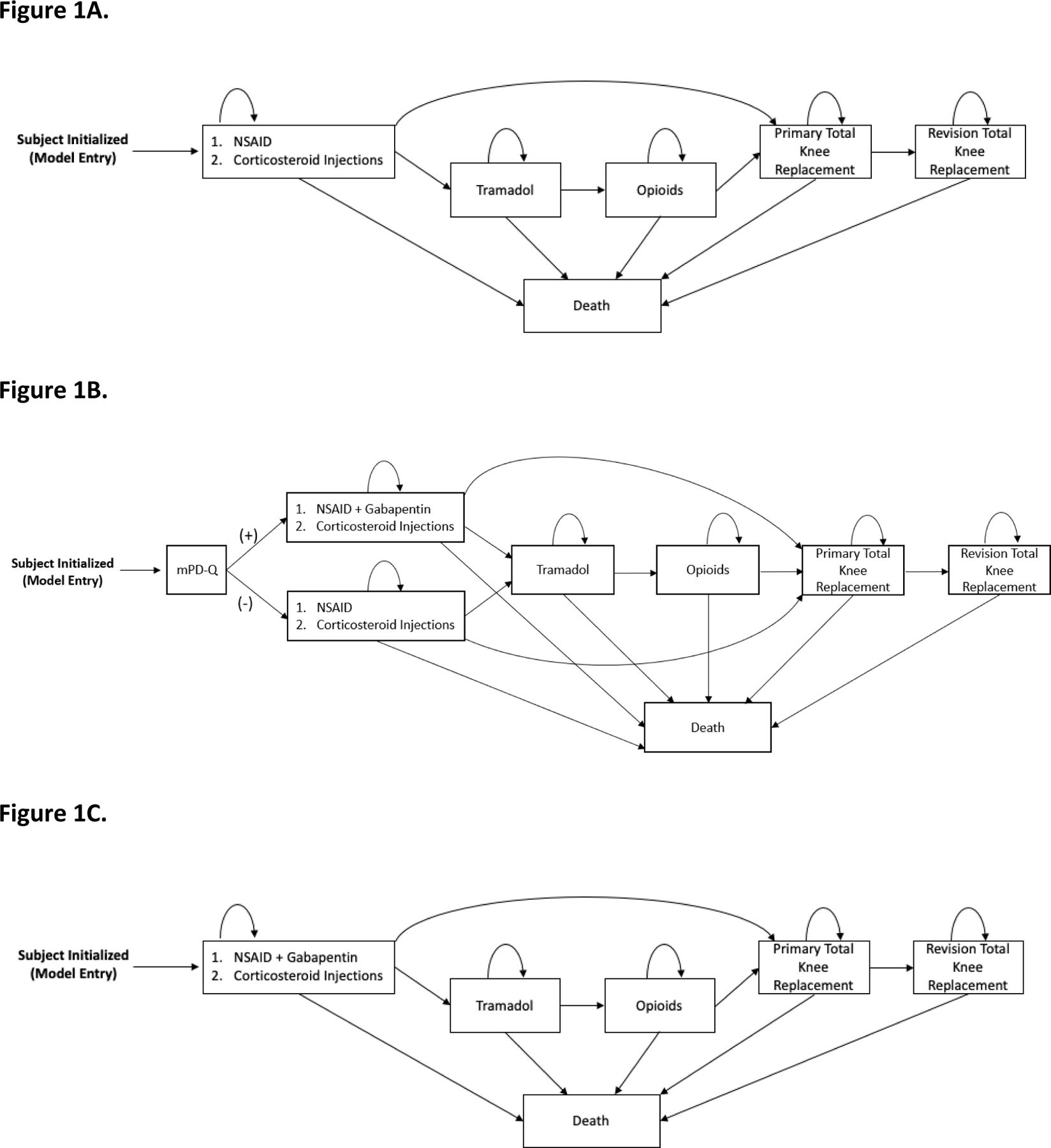
Method: We used the Osteoarthritis Policy Model, a validated Monte Carlo simulation of knee OA, to examine the value of gabapentin in treating knee OA by comparing three strategies: 1) usual care, gabapentin sparing (UC-GS); 2) targeted gabapentin (TG), which provides gabapentin plus usual care for those who screen positive for nociplastic pain on the modified PainDETECT questionnaire (mPD-Q) and usual care only for those who screen negative; and 3) universal gabapentin plus usual care (UG). Outcomes included cumulative quality-adjusted life years (QALYs), lifetime direct medical costs, and incremental cost-effectiveness ratios (ICERs), discounted at 3% annually. We derived model inputs from published literature and national databases and varied key input parameters in sensitivity analyses.
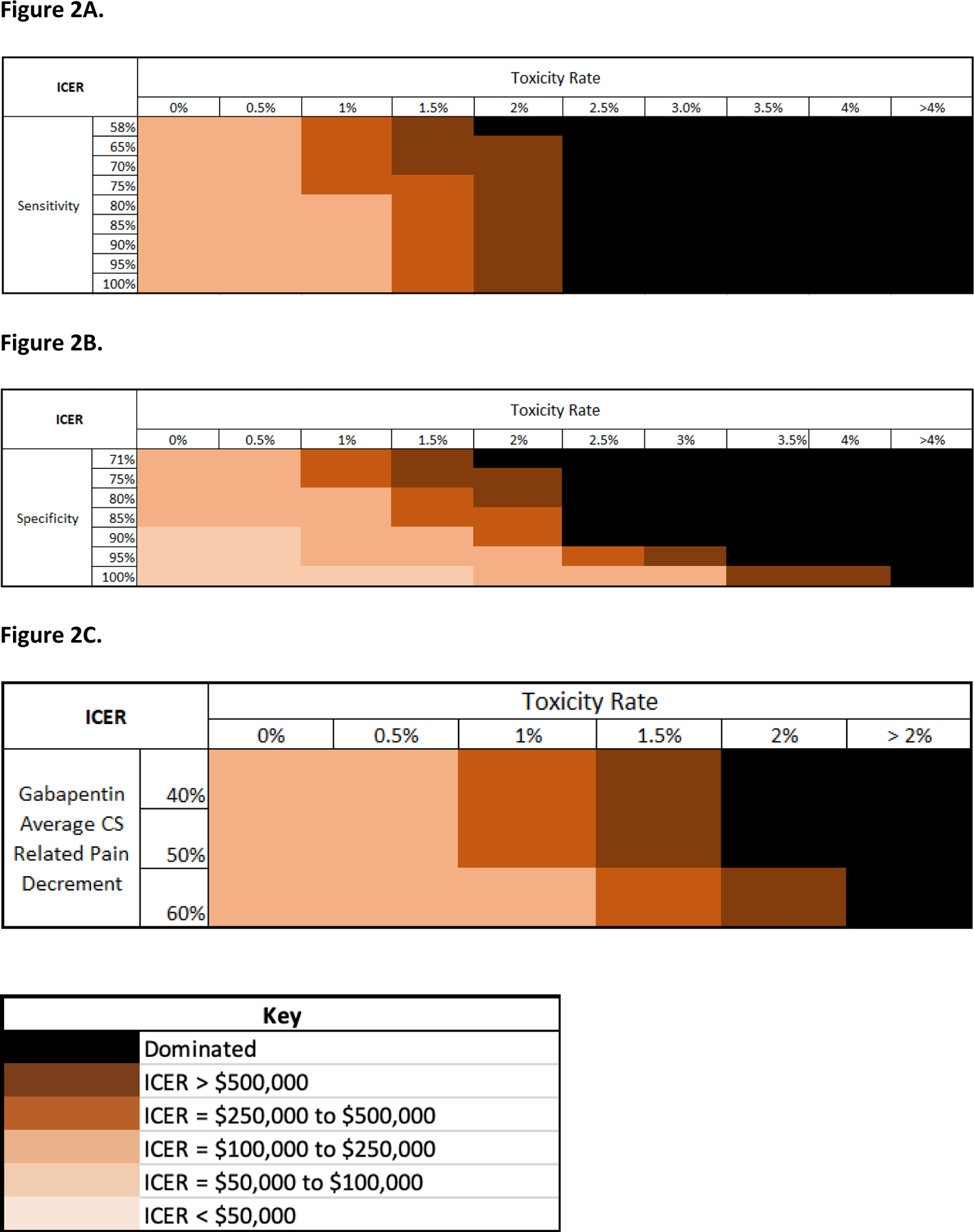
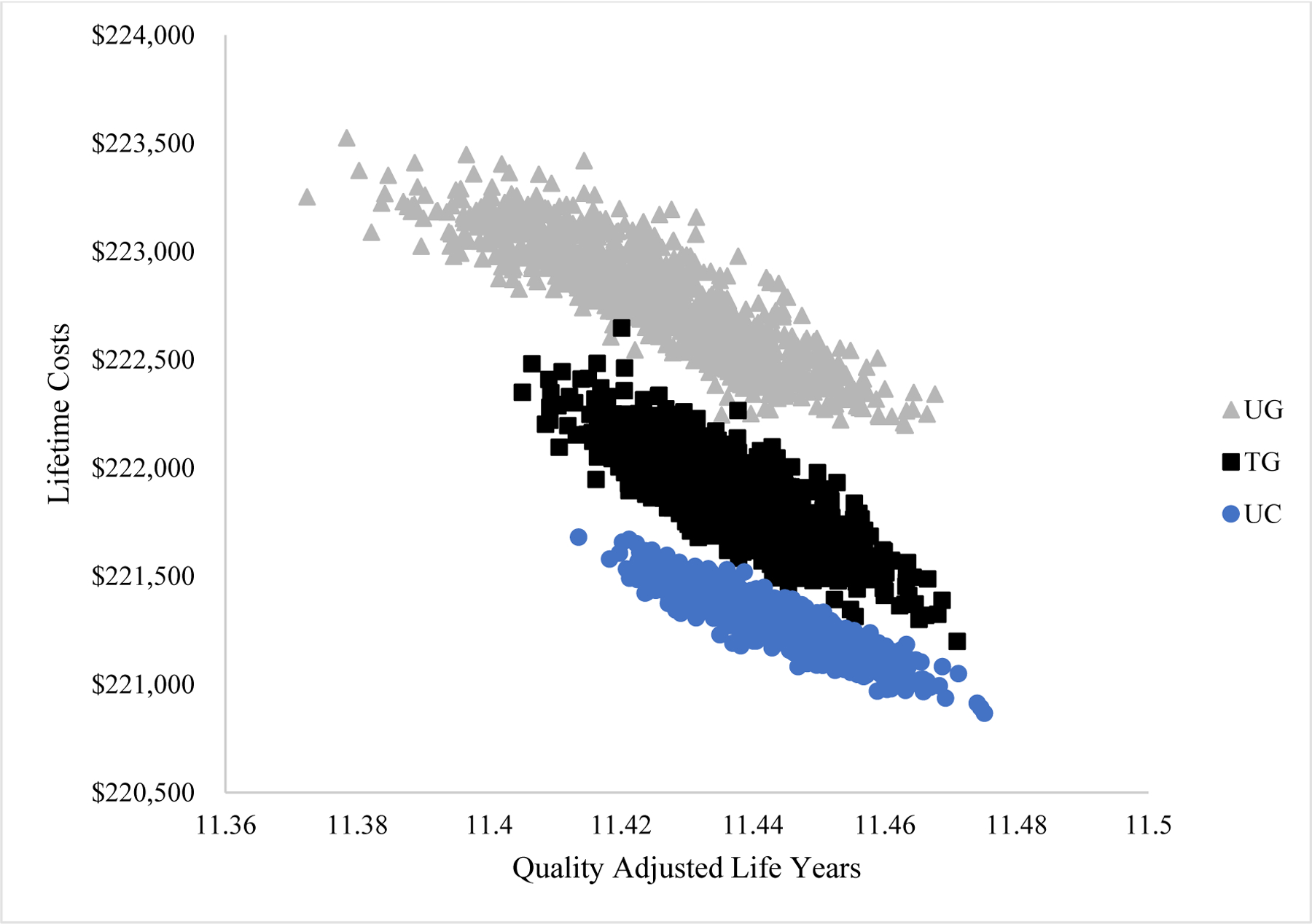
Results: UC-GS dominated both gabapentin-containing strategies, as it led to lower costs and more QALYs. TG resulted in a cost increase of $689 and a cumulative QALY reduction of 0.012 QALYs. UG resulted in a further $1,868 cost increase and 0.036 QALY decrease. The results were robust to plausible changes in input parameters. The lowest TG strategy ICER of $53,000/QALY was reported when mPD-Q specificity was increased to 100% and AE rate was reduced to 0%.
Conclusion: Incorporating gabapentin into care for patients with knee OA does not appear to offer good value.
Keywords: Cost-efficacy; Gabapentin; Knee osteoarthritis; Pain.
Copyright © 2022 Osteoarthritis Research Society International. Published by Elsevier Ltd. All rights reserved.
Conflict of interest statement
Competing Interests
Outside of NIH/NIAMS funding, all authors have not received any other financial support for this manuscript. Outside of this work, Dr. Tuhina Neogi, Dr. Jamie E. Collins, Dr. Jeffrey N. Katz and Dr. Elena Losina currently receive support for research grants from the NIH (Neogi, Collins, Losina), Biosplice (Katz, Losina) and Pfizer (Losina). Dr. Tuhina Neogi, Dr. Jamie E. Collins and Dr. Elena Losina also received consultancy payments from Pfizer (Neogi, Losina), Lilly (Neogi), Regeneron (Neogi), Novartis (Neogi) and Boston Imaging Core Labs (Collins). Gordon P. Bensen, Alec C. Rogers, Valia P. Leifer, Aleksandra M. Kostic, Dr. Robert R. Edwards, Dr. A. David Paltiel and Dr. David J. Hunter have no disclosures.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
